Haemophilia Action UK campaigners march down Downing Street, left the late Ollie Carruthers, Carol Grayson, the late Peter Longstaff, independent campaigner Colette Wintle and her then MP Archie Norman (Image via Colette Wintle early 2000s)
I note the release of the Sir Robert Francis Report looking at a compensation framework for victims of the Contaminated Blood scandal. I thank those involved but urge caution. Some long standing campaigners have yet to give evidence to the Infected Blood Inquiry and that is our focus right now with our legal team at Milners and with Sam Stein our QC. I continue to allege negligence and that the case for compensation goes way beyond a “moral argument”. It is also concerning that in the run up to the report, Sir Robert Francis failed to document the proposals of some activists in meetings held with him, including my own phone conference with fellow campaigner Colette Wintle, fortunately campaigners document everything.
The bottom line is that government must pay compensation for each virus, hepatitis B, C, HIV and any others and adequately compensate infected and affected and the estate of the bereaved. Government must also recognize the repeated REINFECTION of haemophiliacs with multiple deadly viruses each time they injected US factor concentrates manufactured using plasma donations from the highest risk sources. American plasma pools could reach as high as 400,000 paid donors compared to around 25,000 volunteer donors in the UK. Compensation is not a buy one get one free supermarket deal of infections but a recognition of loss and cumulative harm from each virus addressing the needs of each individual and the impact on loved ones.
Haemophiliacs were also exposed to v CJD and they and their families have lived with the anguish of not knowing for decades if they are incubating the prion disease because there is no test available to date.
This week is an important week at the Inquiry as we will be hearing how government failed to respond to key evidence presented in face to face meetings between haemophilia campaigners and ministers in the early 2000s ignoring calls for a public inquiry even as many haemophiliacs lay sick and dying. It is clear activists working jointly with the Newcastle Journal and Chronicle “Bad Blood” campaign were a thorn in the side of government. We now know this from civil servants own comments behind the scenes only recently seen and the impact we were having which led to government making considerable efforts to block proper compensation for victims of the Contaminated Blood scandal for another 2 decades!
Issues discussed at a meeting with Yvette Cooper at Westminster 15th May 2002 included as follows:-
Lord David Owen’s self sufficiency arguement, his financial commitment and concerns over his missing documents.
The Dr J Garrot Allen letter, (1975) warning letter (from the World in Action documentary) regarding the hepatitis risk from using US paid skid -row and prison donors.
The ethics of treatment and the right to “informed consent”, haemophiliacs as guinea pigs, experimentation.
Not adequately informing patients of risks from factor concentrate treatment.
The state of BPL (1979 Inspectorate’s report) and safety concerns and the state of the building.
The use of “hepatitis rich” gay donors in the US, gay donor adsshown.
Arkansas prison plasma collection, information/evidence/photos shown from the sister of a US prison plasma donor, safety violations.
Yvette Cooper working on the Bill Clinton election campaign to the White House.
The Dr Spence Galbraith, (9th May,1983) warning letter to government to remove US treatment from the shelves in the UK due to the risk of AIDS.
Christine Lee policy not to discuss risks with patients mid 1980s.
Use of the safer cryoprecipitate compared to pooled plasma.
Testing for HIV/HCV without permission and with holding test results.
Stigma surround haemophilia and hepatitis C, that of HIV was already well known.
Rise in HCV death figures, misreporting.
The hepatitis waiver in the HIV litigation, (Peter Longstaff’s legal case).
The increased risk of viruses with higher pool sizes.
Conflict of interest with the Haemophilia Society due to funding from pharmaceutical companies.
The importance of all haemophiliacs being offered the safer recombinant synthetic treatmentnot only children.
Pictures shown of Manor House Group member bloated with hepatitis C.
Consumer Protection Act.
Peter Longstaff’s treatment strike, refusing human plasma, Judicial Review case for Recombinant.
Use of paid donors Henan, China scandal.
European Directive, to move away from using paid donors on the grounds of safety.
The need for a public inquiry.
Proper compensation.
The meeting was minuted by Ollie Carruthers for Haemophilia Action UK as we learnt from previous meetings with government, they are often fail to provide minutes. We shared these with the Manor House Group that attended the meeting as well as Haemophilia Action UK and the minutes have been presented to the Infected Blood Inquiry.
It is important to note that far from these issues being “new” as highlighted in recent media by certain campaigners that seem intent on claiming the above as their own work without referencing the research of long standing campaigners, many of the same issues were presented in the mid 1990s and in an earlier face to face meeting Colette Wintle and I had with Lord Philip Huntas well as in countless letters, radio, TV news, documentaries and old newspapers.Both the Hunt and Cooper meetings were attended by Charles Lister who will give evidence this week at the Infected Blood Inquiry, MPs were also present.
Sir Robert Francis will present his compensation report shortly in person to Sir Brian Langstaff, Chair of the Infected Blood Inquiry. The recommendations could be accepted in full, partly accepted or rejected altogether, that remains to be seen. Sir Brian will release his report once all key witnesses are heard and he has compiled his own findings.
Carol Grayson (Haemophilia Action UK)
Carol Anne Grayson is an independent writer/researcher on global health/human rights/WOT and is Executive Producer of the Oscar nominated, Incident in New Baghdad. She was a Registered Mental Nurse with a Masters in Gender Culture and Development. Carol was awarded the ESRC, Michael Young Prize for Research 2009, and the COTT ‘Action = Life’ Human Rights Award’ for “upholding truth and justice”. She is also a survivor of US “collateral damage”.
Don Francis former Centre for Disease Control whose early warnings in the 1980s to exclude gay men from donating blood for fear of infecting haemophiliacs with the AIDS virus were ignored until it was too late(Image via COTT, AIDS conference Washington DC, 2009)
For longstanding haemophilia campaigners that lived through and researched the emergence of the AIDS virus in the early 1980s, it is impossible to forget the delays and denials regarding plasma safety and the alleged incompetence and negligence in terms of donor selection policies and protecting each nation’s blood supply. During the 1970s and 80s, thousands of UK haemophiliacs were infected with HIV and hepatitis viruses through contaminated blood after receiving pooled plasma products named factor concentrates used in the treatment of their inherited bleeding disorder. Some families mourned the loss of multiple relatives as they died of AIDS and liver disease. The contaminated blood scandal is now the subject of the Infected Blood Inquiry chaired by Sir Brian Langstaff.
During the 1960s and 70s, US pharmaceutical companies relied heavily on the use of plasma collected in the poorest areas of Haiti and Central American countries such as Nicaragua and Belize and turned a blind eye to the over bleeding and exploitation of donors selling their blood for a few dollars to feed their families or for their next drug fix. The process of plasmapheresis meant one donor could be bled 104 times each year. Plasmapheresis is described by Healthline as “a process in which the liquid part of the blood, or plasma, is separated from the blood cells. Typically, the plasma is replaced with another solution such as saline or albumin, or the plasma is treated and then returned to your body”
The New Scientist stated in 1975, “as Professor Titmus (author of The Gift Relationship, 1971) highlighted, ‘authorities have drawn attention to the fact that the purchase of blood attracts many alcoholics and other unfortunates who return frequently to blood banks and who know they will be deprived of money if they answer yes to questions about jaundice, malaria, other infectious diseases and hypersensitivity.'”
As time moved on and collection practices in Central America came under closer media scrutiny, public pressure led to the closing of these clinics and a move to focus on new donor communities in the US. Blood collection thrived in American skid row clinics opening up along the US/ Mexican border and the run down areas of inner cities. Pharmaceutical companies turned their attention to utilizing the blood of prison donors and gay men were actively encouraged to donate. Bleeding donors considered high risk for hepatitis viruses became the norm as more and more safety rules were violated.
UK haemophiliacs born with an inherited bleeding disorder where the blood does not clot effectively were reliant on treatment which contained the missing clotting factors. In the 1960s and 70s, haemophiliacs were treated with cryoprecipitate made from a small number of carefully screened British donors. The UK, unlike the US, had a volunteer donor system where people gave blood for altruistic reasons as opposed to financial gain and the British blood transfusion service was considered one of the safest in the world. The level of risk to haemophiliacs all changed in 1973 with the introduction of the so called “miracle” treatment, factor concentrates made from the pooled plasma of thousands of donors and so began the licensing of imported US factor concentrates.
For this particular article the focus is on the use of gay donors and bisexual donors and identify as men who have sex with men (msm). Advertisements published in the US in the gay magazines of the early 1980s show image after image inviting gay men who have had hepatitis B to donate. There was great interest in studying them for a vaccine… however there was also a disaster waiting to happen when the surplus of this so called “hepatitis rich” plasma (of men who sometimes infective) was added to the plasma pools used in the manufacture of factor concentrates.
Don Francis is an American epidemiologist whom this author met in Washington DC in 2009. Francis was at the centre of the emergence of the AIDS virus from 1981. He worked at the Centre for Disease Control and realizing very early on that evidence indicated AIDS was blood borne understand clearly the risk to haemophiliacs receiving plasma products. Blood was often collected in plasma wagons parked outside the bath houses in the Tenderloin area of San Francisco and also from men who took the opportunity to participate in unprotected sex with other men in cubicles even as they waited to sell their blood in US prisons such as Arkansas State Penitentiary. American documentary maker Kelly Duda looked at prison safety violations in his film, Factor 8:The Arkansas Prison scandal.
The link between gay men donating their hepatitis rich blood (hepatitis B being an early marker for the AIDS virus) and the danger to haemophiliacs of becoming infected drove Francis to highlight the need to exclude gay men from donating blood, not to judge their sexual preference but to safeguard the blood supply. What Francis faced however, (portrayed in the film And The Band Played On by actor Matthew Modine) was denial from the pharmaceutical companies and blood bankers unwilling to upset the “gay lobby” and risk unfounded accusations of “homophobia” so they delayed taking action even as the first cases of AIDS emerged in US haemophiliacs that received their blood.
So where did AIDS come from? A History of AIDS, states, “scientists have traced the origin of HIV back to chimpanzees and simian immunodeficiency virus (SIV), an HIV-like virus that attacks the immune system of monkeys and apes.”
Francis described to me at our hotel on Capitol Hill, the moment when he banged his fist on a table in anger and frustration famously asking “how many more have to die” before action was taken to remove gay men from selling their blood albeit wanting to help others but ultimately infecting recipients of their plasma with HIV and hepatitis viruses. In contrast to plasma pools of 20,000 in the UK, plasma pools in the US could reach as high as 400,000 donors as highlighted in Congressional Hearings, add to that the targeting and bleeding of gay men emerging from the bath houses and you were virtually guaranteeing infection.
In a May 1983 article in the Bay Area Reporter, Mike Hippler reported that,
“no one knows what causes AIDS, [but] many are afraid that, like gonorrhea and syphilis, it is communicable, and therefore the baths have come to represent a potential source of contamination. But are the baths a danger zone? … fucking around at the baths, or anywhere is a risk factor, but not a proven cause, says Dr. Dritz (of the San Francisco Department of Health’s Communicable Diseases Department.) But the more intimate contact you have with people, the more chance you have to pick up something from those people, (gay men)’” While individuals for and against closing the bathhouses waged war in the newspapers throughout 1983, 72 San Franciscans died of AIDS complications. Every year the numbers increased. There was panic, from within the queer community and more damagingly from without.”
One gay man contributing his oral history to a San Francisco archive highlighted that before HIV testing was introduced, he would donate blood as a way of demonstrating to others that he was not infected and avoid any stigma associated with being gay. He failed to say whether he was later found to be incubating the AIDS virus or not?
Thousands of haemophiliacs were infected with hepatitis B, C and HIV around the world from US factor concentrates and went on to die as a result of the use of virally high-risk donors and the failure to act quickly enough in removing gay donors among others from the plasma pools. Although there were some early documented cases of AIDS in the UK where haemophiliacs were exposed to the blood of volunteer gay blood donors carrying the AIDS virus, it was much smaller compared to the risk from imported factor concentrates made from the pooled plasma of hundreds of thousands of high risk remunerated donors. Francis can be viewed discussing that time on the following link,
Don Francis Pillars of Democracy, Tainted Blood video
Fast forward 40 years to the 2022, is blood safety still of concern to haemophiliacs?
There has certainly been considerable progress with the widescale introduction of viral inactivation, heat treating blood products and the use of recombinant synthetic clotting factor instead of a total reliance on human plasma derived products. There is also the emerging world of gene therapy. However haemophiliacs are not out of the woods yet. This author was interested to read the following in an article titled, “Plasma or Recombinant products for Hemophilia?” from Ash Clinic News in the US published in 2018, where young children were still being prescribed plasma products, as follows,
The other point I make when explaining plasma-derived products to new patients is that plasma products could reduce their risk for developing inhibitors – an extremely serious complication of hemophilia.
The patient population that I would recommend plasma-derived products to are what we call PUPs, or “previously untreated patients.” That recommendation is based on data from the Survey of Inhibitors in Plasma-Product Exposed Toddlers, or SIPPET trial, that was presented as a plenary abstract at the 2015 American Society of Hematology Annual Meeting and later published in The New England Journal of Medicine.2,3 In SIPPET, we investigated whether the development of inhibitors was related to the type of concentrate used for factor replacement therapy. Of 251 PUPs with hemophilia A enrolled, 125 were assigned to receive plasma-derived FVIII–containing von Willebrand factor (vWF), and 126 were assigned to receive recombinant FVIII with no vWF.
We found that PUPs treated with plasma-derived products had about a 50 percent lower rate of developing inhibitors, compared with those treated with recombinant factors.3 Based on these data, I think the target population for plasma-derived products would be pediatric PUPs, because we want to do whatever we can to limit or prevent the number of inhibitors that occur in patients with hemophilia.
Dr. Dunn: However, treating patients with plasma-derived products requires much higher volumes of products for infusion, compared with recombinant products, which only require a couple milliliters of concentrate. So, if I’m treating pediatric patients, who have tiny blood vessels, with plasma products, I might need to use central venous access devices to deliver the higher volumes of plasma necessary. Implanting a central venous access device, though, means major surgery, which introduces risks associated with anesthesia, infection, and the device itself. If I can ever avoid surgical procedures in patients with hemophilia, I certainly want to do that. I can infuse smaller-volume recombinant products more easily through peripheral veins in pediatric patients.
Dr. Young: The other instance when I would prefer plasma-derived products is in patients who have already developed inhibitors. We also use plasma concentrates when we perform immune tolerance induction therapy, in which we give repeated doses of FVIII to try to eradicate inhibitors.
So not every haemophiliac is receiving recombinant. Some haemophiliacs still receive human factor concentrates which may be related to inhibitors, personal preference or efficacy as some haemophiliacs feel plasma derived products work better for them than recombinant. In addition, haemophiliacs may require whole blood like the rest of the population for accidents, joint operations and liver transplants for those infected with hepatitis C. So we must be ever vigilant regarding blood safety. The haemophilia community and their families are not generally scientists though there may be individual exceptions so are reliant on others to monitor the safety of the blood supply. However through lived experience those that have survived and their loved ones are always looking out for the next virus… to quote former Health Minister Lord Owen, “its not if a new virus comes along but when” and the v CJD prion for example can’t be eradicated in the same way as HIV and hepatitis viruses. In the case of monkeypox now emerging, it is not even a new virus but one that is not often seen outside of west and central Africa and which in the latest infections does not appear to be following its usual pattern/spread of the virus.
The NHS advice regarding “How do you get monkeypox” can be read here as follows:-
How you get monkeypox?
Monkeypox can be caught from infected rodents (such as rats, mice and squirrels) in parts of west and central Africa.
You can catch monkeypox from an infected animal if you’re bitten or you touch its blood, body fluids, spots, blisters or scabs.
It may also be possible to catch monkeypox by eating meat from an infected animal from central or west Africa that has not been cooked thoroughly, or by touching other products from infected animals (such as animal skin or fur).
Monkeypox can also spread from person to person through:
touching clothing, bedding or towels used by someone with the monkeypox rash
touching monkeypox skin blisters or scabs (including during sex)
the coughs or sneezes of a person with the monkeypox rash
As the well respected Nam AIDSMAP pointed out on the 25th May, “the World Health Organization (WHO) has now confirmed nearly 100 cases of monkeypox in over a dozen countries, with the largest number in the UK”. Although it is emphasized that “anyone can catch the virus through close personal contact” the publication also states,
Cases so far have “mainly but not exclusively been identified amongst men who have sex with men,” according to WHO. Among the Global.health cases with a known sex and age, all but three are young or middle-aged men. Many of the affected men identify as gay or bisexual or sought care at sexual health clinics. Several cases are reportedly linked to a sauna in Spain and a fetish festival in Belgium. Many of the men reported recent international travel.
There are now estimated to be around 179 cases in the UK alone and CNBC reports, “globally, 555 confirmed and suspected cases have now been reported in countries outside of Africa.” New guidelines issued are as follows,
U.K. health authorities have urged anyone who tests positive for the monkeypox virus to abstain from sex until their symptoms have cleared.
The U.K. Health Security Agency also recommended that previously infected persons continue to use condoms for a period of eight weeks after the virus has passed to combat rising cases.
It is important to warn men who have sex with men to monitor their health, be aware of the symptoms of monkeypox which can be found on the link below and follow public health advice on reporting and isolating should suspected infection be present.
This is particularly important as Pride months is coming up and this is addressed in an article by Helen Bransworth for StatsNews
“Health officials scramble to raise monkeypox awareness ahead of Pride Month”
But what of blood safety? Who is addressing that? Is there a risk of transmission via blood and blood products and if so how big is that risk? This author is yet to see any comment with regard to blood donation and monitoring blood safety.
The US and the UK were notoriously slow to act on AIDS, especially when it came to excluding gay donors, putting sensitivities over blood safety. This cannot happen again. The public need to know whether donor guidelines need to be reviewed with the new monkeypox cases? Is there a test for monkey pox regarding blood and is it in place? Are there ways of ensuring monkey pox is not present in the blood supply? Would current viral inactivation techniques completely elimate monkeypox?
This author has submitted initial questions to the Department of Health and Social Care and discussed her concerns with fellow haemophilia campaigner Colette Wintle and Kate Burt, CEO of the national Haemophilia Society who can raise questions directly with The Advisory Committee on the Safety of Blood, Tissues and Organs (SABTO) that quote, “advises UK ministers and health departments on the most appropriate ways to ensure the safety of blood, cells, tissues and organs for transfusion/transplantation.” The SABTO website can be viewed on the following link,
For many years there was a blanket ban on msm donating blood but that has recently been lifted in many countries including the UK. Haemophiliacs and their families among the most infected and affected by AIDS through blood and blood products were furious to find out that discussions leading up to the reversal on the ban on gay men donating had excluded them and their representatives from contributing to the ongoing debate over blood safety. Details of the changes and new blood donor guidelines are on the following link,
Landmark change to blood donation eligibility rules on today’s World Blood Donor Day (Blood News, 14th June, 2021)
There is a fear that once again anyone questioning or challenging the current practice of accepting blood from msm will once again be viewed as “homophobic” as opposed to expressing concern over whether current safety practice is adequate and ensuring the safest possible blood supply.
This author has submitted the following questions to the Department of Health on the 21st May 2022,
Dear Sir/Madam,
1) Under a Freedom of Information request, how many cases of monkeypox are in men who have sex with men that have already been immunocompromised with HIV infection?
2) What precautions are the UK taking to protect the national blood supply from monkeypox given that the government recently reversed blood safety policy to include men who have sex with men as blood donors?
With thanks
Carol Grayson
Name and address supplied
This was followed up with further questions on the 23rd May 2022 as follows:-
Dear Sir Madam,
I am writing to you under the Freedom of Information Act to ask the following questions.
1) Whose decision was it to reverse the safety policy on excluding gay men from donating blood to now allow men who have sex with men to donate?
2) Why was this done without any representation from the haemophilia community where the serious failures in delaying excluding gay men led to some haemophiliacs being directly infected with HIV and hepatitis viruses.
3) What improved safety measures are government now considering regarding blood donation policy with the arrival of new cases of monkeypox in men who have sex with men?
With thanks
Carol Grayson
(Name and address supplied)
It now appears that monkeypox may have been circulating in the UK longer than realized and the incubation period is uncertain. Clearly haemophiliacs are once again concerned having been traumatised over and over again, infected with multiple deadly viruses and then exposed to variant CJD (Creutzfeldt-Jakob disease).
Colette Wintle a female haemophiliac wrote to her legal team representing her at the Infected Blood Inquiry and to Kate Talks (Haemophilia Society),
Dear all
Latest reporting on the spread of monkey pox virus and the desperate attempt to disassociate it from the gay/bisexual community to avoid stigmatising them I fear will cause the DOH and other organisations to ignore the bigger picture of risks to the blood supply and once again ignore the rights of vulnerable patient groups like haemophiliacs to be protected.
This has nothing to do with homophobia but it’s a huge and legitimate concern that our safety will be compromised as it was with HIV and hepatitis .during the 70’s 80’s and 90’s.
The reality is that it clearly is being spread by gay / bisexual communities . How do we approach organisations like THT to encourage them to advise the people they represent to avoid donating their blood without becoming a target ourselves of attack? Other than contacting SABTO and the UKHCDO should we try and get a meeting with the Secretary of State for Health? Any thoughts on that? It’s really concerning that nothing has been written so far about advising people who are high risk of being infected to desist from being a blood donor. I am really worried about this situation.
Kind regards
Colette
Unfortunately the government has not helped relationships between haemophiliacs and the Terrence Higgins Trust that represent msm by once again employing “divide and conquer” tactics. THT is a British charity that campaigns about and provides services relating to HIV and sexual health. Haemophiliacs were infected with HIV through their plasma treatment. The reversal on the msm donor ban by government bodies was indeed timely given that the Infected Blood Inquiry is now underway looking at historical infection and past collection of plasma from HIV and hepatitis infected gay donors. Is the government once again attempting to whitewash the “haemophilia holocaust” and draw attention away from the highest risk practices of the 1970s and 80s involving gay donors? The exclusion of the Haemophilia Society and campaigners in the debate ensured there was no honest conversation with haemophiliacs and their families and ensured there was less opposition over reversing the ban on gay donors. Given their horrendous history of infection it is only natural haemophiliacs worry continuously over blood safety.
To add insult to injury, in an act of incredible insensitivity, in recent years, that the government scrapped the Macfarlane Trust set up to provide financial support to HIV infected haemophiliacs and affected families following litigation against the government in 1991 and transferred the remaining funds over to the Terrence Higgins Trust. Although there are gay men in the Haemophilia community, the issues of haemophiliacs are very different to those of msm. Haemophiliac’s issues are focused on historical injustice, alleged negligence, experimentation, treatment with factor concentrates in families where several family members may be infected with multiple viruses and prion exposure (CJD). The haemophilia experience of iatrogenic infection is very different to that of many non haemophiliacs with HIV hence the setting up of the Infected Blood Inquiry. However the pain and suffering of all infected with deadly viruses is recognized by this author and the best treatment and support must be provided for all.
It is important to note that the 1991 haemophilia HIV litigation was kept out of court, no compensation was ever paid but ex-gratia lump sum payments were made to infected haemophiliacs and some infected partners to assist financial need and monthly payments were provided via the Macfarlane Trust including to widows and for children. The trust also set up support week-ends and educational days for families. Years later the Skipton Fund was set up for those infected with hepatitis C and affected families.
However the government made a decision to scrap the trusts despite this author being assured in a Macfarlane Trust meeting of the Joint Partnership Group that the Trust and the monthly payments would remain until the last infected and affected beneficiary died. Suddenly a proposal was put forward to scrap 5 trusts including the Macfarlane Trust and Skipton and amalgamate them under the newly formed English Infected Blood Support Scheme (EIBSS) and its equivalent in the devolved nations. A meeting was held with a government appointed mediator to discuss proposals with haemophiliacs and their families but deliberately excluded long term campaigners so they could not raise objections.
Solicitors that had represented haemophiliacs in the HIV litigation were not informed and only learnt of the changes through their old clients afterwards who were denied the opportunity to seek advice on any legal implications. Some long standing campaigners only found out about the meeting after it took place, nor did they receive questionnaires to complete until it was too late. This author alleges the move to get rid of the Macfarlane Trust was allegedly undemocratic, unethical and possibly illegal. Government lied in public about all Trust beneficiaries/campaigners being consulted. Some haemophiliacs have refused to sign a consent form regarding the transfer of their papers to the Terrence Higgins Trust in protest.
Campaigners accuse the government of “pinkwashing” using THT when haemophiliacs have been extremely outspoken over 4 decades of campaigning on blood safety and issues affecting their community. They do not need THT speaking for them and if the same had been done to THT it is likely they would have been objecting strongly to haemophiliacs taking over THT and claiming to represent msm.
Pinkwashing is a tactic often employed by Apartheid Israel (with whom the British government under Boris Johnson and Keir Starmer, opposition leader are very close).
Pinkwashing is an Israeli government propaganda strategy that cynically exploits LGBTQIA+ rights to project a progressive image while concealing Israel’s occupation and apartheid policies oppressing Palestinians.
Pinkwashing is being used here to divide haemophiliacs and distract away from their voices, giving financial control of Macfarlane monies to the Terrence Higgins Trust instead of the Haemophilia Society. As haemophiliacs await the forthcoming report from Sir Robert Francis on a compensation framework for those infected and affected, the voices of long standing haemophilia campaigners are being watered down on what they actually want. They do not need THT speaking for them or determining the agenda. Government must address those infected and affected through contaminated blood directly. Haemophilia representation comes through joint working with their legal representatives and the National Haemophilia Society not THT or the APPG for Haemophilia and Contaminated Blood that sat on key evidence and awarded research for years, damage limitation for government?
THT recently announced that on the agenda of the next Macfarlane Conversation would be the following,
As part of Terrence Higgins 40th Anniversary, how we mark 40 years since HIV and haemophilia was first linked?
Is this a deliberate ploy to cause further distress to the Haemophilia community who were often infected through the blood of gay men as highlighted in US legal depositions and then had their HIV Macfarlane Trust allegedly illegally scrapped and passed over to THT. That will be quite some conversation!
This author does however recognize the positive work carried out by THT in some non haemophilia areas and indeed provided a quote in support of stopping cuts to services in parts of London, highlighting THT as follows,
“Community HIV services provide invaluable support and are a lifeline to those living with HIV that still suffer prejudice and discrimination. Cuts to these services at grassroots level is false economy as it means vulnerable persons will be missed or picked up much later and that could incur greater costs to hospital services. It makes no sense to remove key funding when HIV rates are above the national average in Lambeth, Southwark and Lewisham. Charities such as the Terrence Higgins Trust with decades of experience provide essential practical support and give guidance on benefits and housing as well as being there for the increasing numbers now struggling in poverty. THT also offer important counselling services. Having good support helps people to feel valued and to maintain independence in day to day living. Withdrawing funding is a very backward and unwelcome move and will cause unnecessary suffering to those infected.”
So far however most former Macfarlane Trust beneficiaries have not seen a penny from THT that appear inflexible on grants wanting only to give funding for counselling with requests regarding other needs turned down. It is surely time for THT to butt out of haemophilia campaigning and politics and stop using haemophiliacs as a means to attract additional funding.
This author has submitted the following previously unanswered questions regarding the scrapping of the Macfarlane Trust and transfer of funds to THT to the Department of Health, dated 30th May, 2022,
Dear Sir/Madam,
1) Under Freedom of Information please provide any documents discussing, or relating to the transfer of the Macfarlane Trust funds to the Terrence Higgins Trust (THT)
2) What was the reason THT were chosen as they are a sexual health charity with a history of specialising in the support of men who have sex with men? (Especially given the fact that many haemophiliacs were infected with HIV and HCV and died following the delays in excluding gay men from the plasma pools as highlighted in litigation testimonies.)
3) Why weren’t funds transferred to the Haemophilia Society that understand the needs of haemophiliacs with HIV/HCV and have a history of grant making to haemophiliacs?
4) Why did the government give false statements saying all haemophiliacs were included in the consultation to scrap the Macfarlane Trust and Skipton Fund when long standing campaigners of 30 years that had sat on the Joint Partnership Group of the Macfarlane Trust were deliberately excluded from the meeting with a government mediator to discuss their views?
5) Why were some campaigners not sent questionnaires until it was too late for them to submit their views.
6) Why was the process of consultation regarding scrapping the trusts both undemocratic and discriminatory?
7) Who made the decision to transfer Macfarlane Trust monies to the Terrence Higgins Trust?
With thanks
Yours sincerely
Carol Grayson
Address supplied
To return to monkeypox and blood safety… how has government response varied in relation to men who have sex with men and haemophiliacs? Within the last 3 weeks as monkeypox has emerged, there has been a quick response from government to advise msm on prevention and what to do if infected. On June 2nd, Reuters highlighted,
According to the UKHSA, the majority of cases in the United Kingdom – 132 – are in London, while 111 cases are known to be in gay, bisexual, or other men who have sex with men (GBMSM). Only two cases are in women.
Recent foreign travel to a number of different countries in Europe within 21 days of symptom onset has been reported by 34 confirmed cases, or about 18% of the 190 cases of the disease that have been confirmed by the United Kingdom as of May 31.
So far, the UKHSA has identified links to gay bars, saunas and the use of dating apps in Britain and abroad.
“Investigations continue but currently no single factor or exposure that links the cases has been identified,” the agency cautioned.
Monkeypox can affect anyone, but many of the most recent diagnoses are the GBMSM community – many of whom live in, or have links to London, said Kevin Fenton, London’s regional director for public health.
There has not been one single statement from government so far to reassure the haemophilia community regarding current blood safety and no attempt whatsoever to engage with campaigners to try to allay any fears. Once again haemophiliacs are a forgotten community put on the backburner. It is unlikely government will want to draw further attention to past blood safety violations with the contaminated blood compensation framework proposals about to be released and with the recent changes to allow msm to donate (deemed controversial by some). If past experience is anything to go by, government will continue to be focused on denying culpability, minimizing payments to the those infected and affected and reneging on commitments given to provide “substantial compensation”. Nor will government want today’s blood safety guidelines placed under direct scrutiny in relation to monkeypox and msm just in case once again they have failed us!
Carol Anne Grayson is an independent writer/researcher on global health/human rights/WOT and is Executive Producer of the Oscar nominated, Incident in New Baghdad. She was a Registered Mental Nurse with a Masters in Gender Culture and Development. Carol was awarded the ESRC, Michael Young Prize for Research 2009, and the COTT ‘Action = Life’ Human Rights A
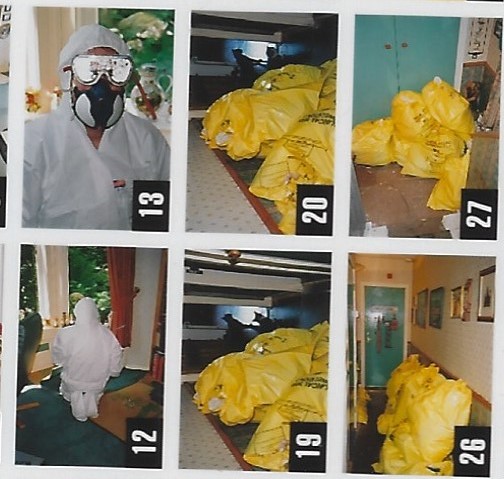
Men in biohazard suits remove carpets due to risk of v CJD contamination at the home of haemophiliac Peter Longstaff after a burst vein (Image Grayson, archive)
The history of variant CJD exposure in haemophiliacs given factor concentrate treatment (pooled plasma products) for an inherited bleeding disorder and the fight for Recombinant synthetic treatment are very closely inter-twined. As soon as they became aware that vCJD could be in the UK blood supply, they knew they were at risk and must look for an alternative treatment.
On the 15th February 1996, the Independent newspaper ran a short article with the headline BSE “cause of death” where a Newcastle virologist Dr Harash Narang was making an extraordinary claim and that was that, “Mad Cows Disease” could be passed on to humans, the article stated,
Peter Hall, of Chester-Le-Street, Co Durham, died last week just days before his 21st birthday after being ill for two years.
Dr Harash Narang, a clinical virologist formerly with the public health laboratory service, said last night Mr Hall had died from Creutzfeldt- Jakob Disease, while Mr Hall’s parents, Derek and Frances Hall, called for more tests to be carried out.
The official Government view is that Mad Cow Disease – or bovine spongiform encephalopathy (BSE) – cannot be transmitted to humans.
Just a month later, on the 20th March 1996, SEAC (Spongiform Encephalopathy Advisory Committee) announced a probable link between BSE in cows and vCJD in humans where 10 cases were reported.
For Peter Longstaff, born with severe haemophilia (less than 1% clotting factor) and this author (his wife), this was a very worrying development. For some years they had watched news reports of distressed and sometimes suicidal farmers, staggering cows with BSE and burning pyres as herds of cattle were destroyed to avoid contaminating the food chain. John Gummer, agriculture minister, 1989-93 was famously seen back in 1990 feeding his daughter a beef burger to help restore public confidence but the public were becoming more and more alarmed.
The current NHS website last updated in 2021, states,
There’s clear evidence that variant CJD (vCJD) is caused by the same strain of prions that causes bovine spongiform encephalopathy (BSE, or “mad cow” disease).
In 2000, a government inquiry concluded that the prion was spread through cattle that were fed meat-and-bone mix containing traces of infected brains or spinal cords.
The prion then ended up in processed meat products, such as beef burgers, and entered the human food chain.
On the 29th March 1996, Longstaff wrote to his then Consultant Dr Peter Jones, Royal Victoria Infirmary, Newcastle, requesting Recombinant, as opposed to human plasma products from UK Blood Products Laboratory (BPL) which it was feared might contain the prion vCJD. This letter has been submitted to the Infected Blood Inquiry chaired by Sir Brian Longstaff who is looking at how haemophiliacs (including Longstaff and his younger brother) came to be infected with HIV and hepatitis viruses through their plasma treatment which included products imported from the US from “high risk” donors, such as prisoners, gay men and prostitutes.
Longstaff was turned down for Recombinant on the grounds of cost (Recombinant could be twice as expensive as human factor concentrates and what we learnt years later was that in the Autumn of the same year (1996) he had 12 exposures to vCJD then classed as “a relatively new and rare neurological disease, classified as a Transmissible Spongiform Encephalopathy (TSE)”.
Although it was years before Longstaff learnt of his exposure to vCJD, we later discovered that haematologists had published a paper in the Lancet about the risks to patients and on the 1st December 1997, Nature Journal, ran with the title, UK accused over risk of CJD in plasma and highlighted the following,
Foot-dragging by the British government is exposing haemophiliacs to an avoidable risk of infection with the new variant of Creutzfeldt-Jakob disease (vCJD) from contaminated blood products. That was the warning issued last week by the organization that represents the directors of 109 centres that treat haemophilia and other complex blood diseases.
The government has acknowledged that blood products pose a potential risk of transmission. But it has so far limited action to commissioning a detailed risk assessment of the problem, and asking the National Blood Authority to consider removing lymphocytes from the blood, given that the causative agent of vCJD may occur in these and other lymphoreticular tissues (see Nature 390, 105; 1997).
In a letter to The Lancet, however, the UK Haemophilia Centre Directors’ Organization says the potential risk is already obvious. It calls for immediate action to protect haemophiliacs by switching them from blood products prepared from UK plasma supplies to either recombinant alternatives or products prepared from donor plasma collected in countries with no recorded cases of bovine spongiform encephalopathy (BSE) or vCJD.
The potential risk to patents was also stated…
The potential risk for haemophiliacs is much higher than for other transfused patients, as they receive multiple transfusions of products prepared from pools of plasma derived from 20,000 to 50,000 individual donations. “There is therefore obviously a much increased risk of getting at least one infected donation in the pool, and one batch of factor VIII may go to 50 haemophiliacs,” says Ludlam.
The article concluded,
Ludlam’s frustration is shared by many researchers who feel that the risk from blood products is receiving insufficient attention. “I took part in the discussion in the early 1980s over HIV and blood, and I have that awful sinking feeling all over again; the issues are so similar,” says Ludlam. “All we need is one haemophiliac to get vCJD and all blood products will be removed from the market.”
The following year 1998, when Longstaff continued to request Recombinant, the BMJ stated that the trust refusing to provide Longstaff with safer treatment, was “following the Department of Health’s guidelines issued in March 1998 that only patients with haemophilia A aged under 16 and those not previously treated with plasma based blood clotting products should be given the genetically engineered recombinant factor VIII.”
Moving on to the year 2000, by chance, Grayson read a letter on v CJD in the Newcastle Journal from Dr Harash Narang who had worked at the Public Health Laboratories in Newcastle. Grayson responded in writing and this was noticed by health journalist Louella Houldcroft who wanted to learn more about what had happened to the haemophilia community. After meeting Grayson and Longstaff, she then invited them to work jointly with her to set up the “Bad Blood” campaign, seeking truth and justice for haemophiliacs given contaminated blood.
Grayson and Longstaff also met up with Dr Narang. To their surprise he stated he already recognized Longstaff’s name from the Newcastle labs as he had tested his blood for hepatitis C. What Longstaff learnt from Narang, was that this occurred years before he knew he was being tested. Seemingly blood had been taken to check clotting factor levels in the blood but was used without his permission to test for HCV in 1992 and apparently before this date. Longstaff was only told he was positive in 1994 in the presence of his wife.
Regarding BSE, Narang explained that he had teamed up with a local business man, Ken Bell, who was in the meat trade and had offices just a 7 minutes walk from the couple’s home. Bell was also concerned about BSE and inadequate safety regulations and was now sponsoring Narang’s work.
Back in 1996, on the 10th January, the Independent wrote about Narang, who was viewed as a controversial figure by some but was sought out by the families of those already dying from what became known as variant CJD. He felt the government were covering up over BSE and the use of MBM so as not to have a negative impact on the British beef industry. MBM refers to meat and bone meal given to cows that are herbivores, eating grass. They have one stomach with 4 compartments for this process and were never meant to eat meat. Milk Means More website explains the process of digestion for a cow as follows:-
Parts of a cow’s stomach:
Rumen – This is the first part of the cow’s stomach. It helps break down complex plant products like grass.
Reticulum – Here the food mixes with the cow’s saliva and produces cud. Cows burp up the cud into their mouths and chew it to help break it down more. When you see a cow that looks like she is chomping on bubble gum, really she is chewing her cud.
Omasum – Here all the water is absorbed out of the food.
Abomasum – Here is where the food is finally digested, similar to what happens in a human stomach.
The Independent wrote on the working relationship between Narang and Bell stating,
Harash Narang, a clinical virologist at the Public Health Laboratories in Newcastle upon Tyne, was the man Mr Bell chose to sponsor. Having done much original work on spongiform disease over 25 years, Dr Narang had devised a slaughterhouse test to diagnose BSE in cattle that hadn’t yet shown clinical symptoms of the disease. But in 1990 when he applied for an official grant to develop the tests, he was turned down. Beef was safe, the Ministry of Agriculture told him.
Mr Bell was incensed: “Here was a scientist who had some answers. Someone who was prepared to meet the problem head on. And yet the old boy network wouldn’t let him work on the test. They didn’t want some little Indian guy to come along and prove them all wrong.”
Mr Bell offered Dr Narang pounds 20,000 to develop two cattle tests. “I want to be able to practise ‘due diligence’ when I trade meat,” Mr Bell explains. “The sooner BSE is weaned out of the cattle market, the better.” There is also a personal motive behind Mr Bell’s crusade: his brother, a butcher, died in 1983 of a dementing brain disease. “He ate a lot of animal heads”, is all Mr Bell will say on the matter.
Bell did however make a comparison between the safety of British beef and that from Namibia stating,
Namibian beef has a better flavour and is reared naturally, he says: no forced fattening, no dark sheds, no dangerous chemicals. And he says he can guarantee that it is BSE-free. The British beef industry, by comparison, is in a mess and as a meat trader he wants no part in it.
“We are feeding cattle diseased food, then feeding diseased meat to our people … I know some meat traders feel that I have betrayed the industry, but I believe you have to sell what is safe. I don’t know if BSE can be passed on to humans. But I’m not prepared to find out by carrying out an experiment using real people.
A government inquiry into the BSE scandal in 2000 deemed as a whitewash” by some did conclude as mentioned earlier that the spread of BSE “may have been amplified by the feeding of contaminated MBM to cattle.” Those eating BSE contaminated meat then became infected with variant CJD who then donated their blood without realizing their status. These new blood safety concerns prompted Longstaff to begin a very public treatment strike refusing any human plasma to treat his haemophilia.
Narang was keen to further his own research into vCJD but claimed to have been hounded out of his job because he knew too much and because of racism. Among other claims of his were that cases of BSE were known years earlier than government had announced and that he was being blocked on developing a test for vCJD and that his character was being deliberately defamed to silence him. A year before we met Narang, the Independent had now run another very different story on the scientist, expressing doubt over his findings, detailed below,
“ How a scientist obtained thousands for a BSE test he could not prove”
In 2000, the Observer reported that France was so concerned over the health risk from beef they were threatening to sue over BSE,
With most British and French experts agreeing that BSE was a disease ‘exported’ from the UK to France, lawyers believe there would be a case for French families of variant CJD victims to sue the British government
and
The Philips BSE report published last month confirmed that the spread of the disease was most probably caused by animal feed made from meat and bone meal which contained infected cattle. Britain banned the practice in July 1998, but figures from Customs and Excise reveal that in 1989 France imported more than 15,000 tonnes of meat and bone meal (MBM). By 1990, the amount had dropped to just over 1,000 tonnes and to practically zero the year after.
In 2001 the following appeared in the press, detailed in an old email of this author,
One of the government’s vCJD advisers, Prof. Michael Banner of King’s College in London, said the handing of the situation was a shambles. He said the government was seriously misleading the public about the risk of vCJD because the incubation could be as long as 20 years.
It is important to note that although over 800 haemophiliacs were exposed to vCD through blood from a donor with the prion, due to delays in notifying haemophiliacs that they could be harbouring v CJD which has a very long incubation period, they had no representation at the Philips Inquiry in 2000. There was no test available which could identify those that had vCJD and it was years before most haemophiliacs were notified of their exposure.
The result of cheap cattle feed, BSE in cows, people eating infected beef, donating blood even as they unknowingly incubated vCJD put the national blood supply at risk as Brits could no longer use UK plasma and safety restrictions had to be put in place. This was played down as the beef industry was already nearing collapse over BSE with famers committing suicide and in addition the nation’s blood supply was now compromised through careless policy and the unethical practice of cannibalising cows!
The symptoms of v CJD can be read on the following NHS link.
Soon after the Philips Inquiry reported, Grayson was sent a leaked letter stating that haemophiliacs had been exposed to v CJD but “don’t tell them” plus she obtained a 4th of November 1997 product recall letter from BPL containing affected factor concentrate batch numbers given to haemophiliacs.
At this time, Longstaff and Grayson began phone and e-mail contact with Frances Hall, the mother of Peter Hall, who died aged 20. Hall campaigned on vCJD and they were introduced to other families who believed there was a massive cover-up over BSE, vCJD. In many ways this echoed the Contaminated Blood scandal putting profit before safety, cheap feed for cattle and cheaper plasma products for patients at the risk of their health. Grayson and Longstaff were also in touch with Professor Ironside at the CJD Surveillance Unit in Edinburgh.
A Journeyman video from 2000s can be viewed on the following link which paints the picture of the time, a country in fear over the BSE crisis. Dr Narang can be seen on the video.
BSE: Biting the hand that feeds you
Longstaff began his legal fight for Recombinant, access to which had become a “post code lottery” with treatment being phased in by age, aimed at the children first. Longstaff fully supported the children having early access but he also wanted to speed up access for haemophiliacs that were already suffering badly due to their earlier infections with HIV and hepatitis C. Thus began a series of letters back and forth to their local Health Authority pleading for the safer treatment with well reasoned arguements but although some doctors supported the couple, the answer from managers was always in the negative. In exasperation, Longstaff launched a Judicial Review in the High Court.
Haemophiliac patient goes to High Court to get synthetic factor VIII
The case came to be heard in 2003. The Northern Echo reported,
As a result of contracting various infections whilst being treated at the Royal Victoria Infirmary, Newcastle, Mr Longstaff decided in 2000 to refuse further treatment with Factor VIII derived from human blood plasma – made from thousands of individual blood donations – on the grounds that it had proved impossible to guarantee the safety of the product.
At a recent hearing, a judge was told the case was urgent as his situation was ”gradually deteriorating” and time was important.
The judge also heard 95 haemophiliac patients treated at the Royal Victoria Infirmary, Newcastle, had tested positive for HIV infection in recent years, and 78 had died.
Mr Longstaff was in ”the surviving group of 17”.
He had also contracted hepatitis B, diagnosed in the mid-1980s, hepatitis C in 1994. Hepatitis G and the HIV Aids virus were diagnosed about 1985.
Although the judge understood and was sympathetic to the reasons why Longstaff was refusing treatment and wanted a safer alternative to human plasma, he explained that if he allowed his case to go through, it would open the floodgates far beyond haemophilia to other treatment areas.
During this time, the couple met James Meikle from the Guardian, who wrote extensively on BSE and vCJD. They began to collaborate on articles and the couple shared letters regarding their fight to ensure there was no cross contamination to or from others when medical instruments were used in hospital. The government looked at single use instruments however the alternative did not go down well with doctors who found them less precise and at least one death was reported.
A policy was then devised to put haemophiliacs exposed to vCJD at the end of the day for invasive hospital procedures keeping one set of instruments for those incubating or exposed with vCJD. It is much more difficult to kill a prion compared to HIV or hepatitis C so Grayson was concerned that her husband might be exposed to vCJD yet again if the same instrument was used on multiple persons with vCJD. Meikle went on to win a first prize…the General Medical Consumer News category at the prestigious Norwich Union Healthcare Medical Journalism Awards 2003 for his piece on CJD.
On the 6th September, 2004, Grayson wrote a long email to a journalist writing on v CJD, one passage detailed a recent incident that showed how little the government had prepared haemophiliacs and their families to deal with their exposure,
I do have real cause for concern, my husband recently had a burst vein resulting in blood spillage, and the advice from professional organizations on dealing with blood spillage because of concerns over vCJD in blood was to send two men in full bio hazard suits to our home to remove our carpet which was then sent to be disposed of at a special incinerator in Leeds. I photographed the whole operation and this appeared on a local BBC News feature. As a carer of a severe haemophiliac who sometimes bleeds copius amounts of blood, I have still not received guidelines on how to deal with a blood spillage in the community with regard to v CJD risk, yet there are guidelines for hospitals and guidelines on how to deal with HIV, hep C blood spillage in the community. This incident was referred by infection control at our local hospital to the CJD incident panel about a year ago. I am still waiting for guidelines for blood spillage in our community.
Through the early 2000s Grayson and Longstaff did many media articles on vCJD and Grayson established positive contact with the Liberal Democrats, in particular the late Patsy Calton MP. On 22nd September 2004, the Guardian published an article titled, Lib Dems call for v CJD blood inquiry, this was announced at their yearly conference, the paper stated,
The Lib Dems call for an inquiry into transfusions comes after it was announced that patients who received blood products from donors who subsequently died from vCJD were to be warned they could be carrying the disease.
The measures are being taken after it emerged last year that a patient had died after a transfusion from someone with the disease.
That was thought to be the first time vCJD has been transmitted from person to person.
The conference also heard concerns over the handling and treatment of donated blood, the failure to alert patients to known risks and the failure to take action when the risks become apparent.
Junior Lib Dem health spokeswoman Patsy Calton said all those affected by the contamination of blood products, including haemophiliacs put at risk of exposure to HIV and hepatitis C, as well as vCJD, were entitled to an inquiry.
“The families of the over 780 individuals who died as a result of the failing in blood products deserve answers,” she said.
“To provide closure to the victims and to ensure there are no further scandals in this area, the government should hold a full independent inquiry into the failures of the past.”
An early day motion was also circulated by the Libdems as follows:-
Motion text
That this House notes the severe illness and deaths of haemophiliacs and some partners from HIV and hepatitis C, caused by the use of contaminated blood products, and the potential for future deaths from vCJD; and supports the Haemophilia Society in its call for an independent public inquiry into the contamination of haemophilia treatment since the 1970s, in particular the failure to make the UK self-sufficient in blood products, the failure in some parts of the UK to make a timely switch to virally inactivated treatment when this became available from 1985 and the failure to make timely provision of genetically-engineered recombinant Factor VIII and IX for all haemophiliacs.
Just 2 days later, 26th September 2004, the Guardian reported… CJD risk letters go to 6,000 patients. Haemophiliacs that had not already hounded their doctors like Grayson and Longstaff to find out if they had been exposed to the prion, received official letters asking them if they wished to know if they had been exposed or not and directions for how to proceed.
On the 13th October 2004, reports appeared in the press with regard to Grayson contacting the Food and Drug Administration (FDA) after she discovered an English and French case where Europeans had sold their blood in the US this compromising the safety of the US blood supply regarding vCJD. UPI, reported,
The Agency’s William Freas, who serves as Executive Secretary of the TSE Advisory Committee, confirmed he received Grayson’s remarks, but said it was up to Committee members whether her concerns would be discussed at the meeting.
They’re going to receive her concerns, but the individual members are independent from the FDA and only they can decide whether to discuss the issues raised by Grayson. Freas told UPI, he couldn’t say anymore due to FDA’s very tight restrictions on what we can say” before advisory committee meetings.
Grayson said in her letter she is concerned that if any of the foreign nationals who donated blood or plasma in the United States do subsequently develop vCJD, US patients who received the blood or blood products derived from their donation may never be notified,
In 2005, Recombinant was finally phased in for haemophiliacs of Mr Longstaff’s age group. Despite a sustained and exhausting effort, he never got his safe treatment and died in a hospice with his wife beside him not long after his 47th birthday. His last selfless act had been to organize for his brain and other tissue to be donated to the CJD Surveillance Unit at Edinburgh for research to be carried out by Professor Ironside in order that other haemophiliacs might benefit and increase their knowledge of vCJD.
Last week at the Infected Blood Inquiry, it was distressing to those infected and affected to hear v CJD being portrayed as an “accident”. This is far from reality. A series of choices led to to vCJD and a crossing of unethical and unnatural boundaries in the use of MBM feed. If this is not examined and accepted then how do we know something similar won’t happen again?
This week it is Professor Ironside giving evidence. He is remembered as being approachable, helpful, and willing to give his time. I hope those listening will hear some of what Phillips failed to deliver in 2000, only with truth and justice can haemophiliacs and their families begin to heal and finally find some peace.
Link
800 HAEMOPHILIACS GIVEN TAINTED BLOOD AT RISK OF VCJD (Independent, 20th May, 2009)
Carol Anne Grayson is an independent writer/researcher on global health/human rights/WOT and is Executive Producer of the Oscar nominated, Incident in New Baghdad. She was a Registered Mental Nurse with a Masters in Gender Culture and Development. Carol was awarded the ESRC, Michael Young Prize for Research 2009, and the COTT ‘Action = Life’ Human Rights Award’ for “upholding truth and justice”. She is also a survivor of US “collateral damage”
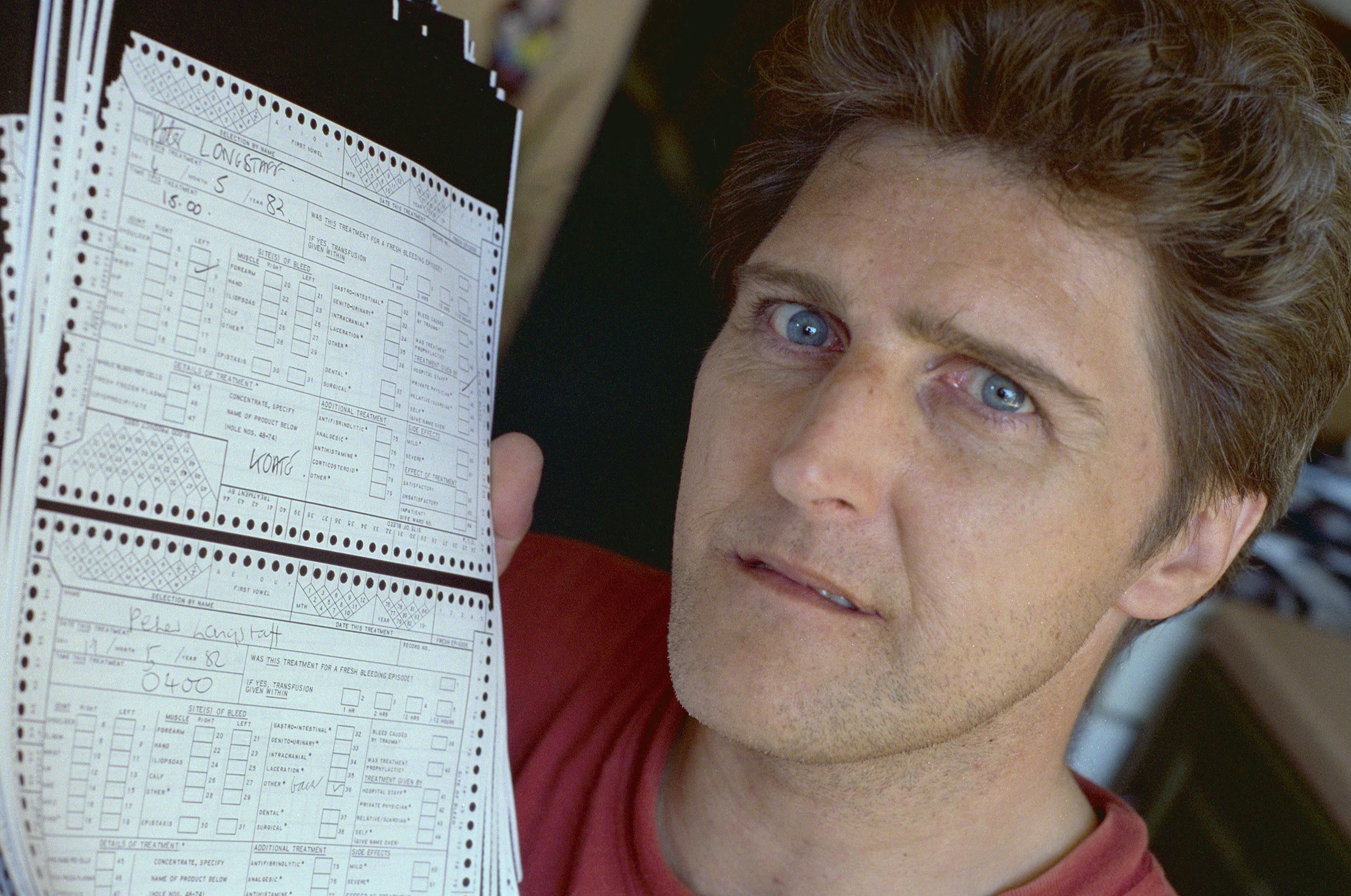
A scandal lasting decades. Peter Longstaff, deceased, a litigant in the 1991 HIV litigation which contained thousands of documents also detailing the hepatitis risks never shown to claimants
Dr Peter Kernoff, was a well renowned Consultant Haematologist who had worked at both the Oxford Haemophilia Centre and the Royal Free Hospital in London. Under his care were haemophiliac patients born with a disorder where there blood does not clot. In order to treat their hereditary condition, haemophiliacs were often treated with American clotting factor concentrates manufactured from the plasma of paid donors. During the 1970s and 1980s this was sourced from “high risk” donors including prisoners, prostitutes and gay men often carrying deadly viruses.
In the Spring of 1983, Kernoff, made a spectacular miscalculation regarding the danger of the AIDS virus in US factor concentrates. In a now infamous interview in a Haemophilia Society publication, Kernoff was asked about the risk of AIDS. This was at a time when experts in the US such as Dr Donald Francis, an epidemiologist at the Centre for Disease Control were warning in 1982 that it was very likely the AIDS virus could be transmitted through blood products which meant haemophiliacs were at great risk. In fact the first cases in haemophiliacs in the US were already emerging that same year.
Kernoff was asked,
Question… Could haemophiliacs get AIDS?
He replied,
Answer… Of course its possible. But I’d expect AIDS to remain a rare disease. The idea that there’s an epidemic of AIDS among haemophiliacs is ludacris.
In an interview with the Northern Echo on 14th March 2018, Carol Grayson, longstanding campaigner/researcher and widow of haemophiliac Peter Longstaff who died after being given contaminated blood infected with HIV and HCV, highlighted how AIDS warnings were missed by UK haematologists including Kernoff and the British government in January 1983. They had already ignored the 1982 concerns. See following link,
Widow claims Contaminated Blood warnings were missed
Recently, Dr Andrzej Rejman, who was a Senior Medical Officer at the Department of Health (responsible for Haematology) from 1989 to 1987 gave evidence as a witness to the Infected Blood Inquiry chaired by Sir Brian Langstaff. The Blackpool Gazette reported that,
Experts looking into the impact of the blood scandal, which saw up to 30,000 NHS patients infected with HIV and hepatitis through contaminated blood transfusions in the 1970s and 80s, were asked to ‘tone down’ their reports, a court has heard.
It is with some interest that this author also notes a letter dated, 22nd February 1991 detailing the contact between Rejman and Kernoff posted on the Facebook page of the Factor 8 group where Kernoff is informing Rejman of a couple of writs he received in relation to hepatitis infection.
This author has long highlighted over decades that haemophiliacs including her late husband were never told the hepatitis risks of their treatment so they could make an “informed” decision whether or not to take factor concentrates. (The same happened when the AIDS risk emerged.) The withholding of key evidence on the dangers of hepatitis C (previously known as non-A, non-B hepatitis) during the time of the 1991 HIV litigation was backed up by a legal opinion from Matthias Kelly QC, the former Head of the Bar Association who saw key HIV litigation documents provided by Grayson and her late husband Peter Longstaff in the early 2000s. On reviewing the signing of a now infamous hepatitis “waiver” within the litigation settlement which prevented haemophiliacs (who were not even tested for hepatitis C at the time) from taking a legal case for their infection, Kelly concluded the following,
Tony Mallen solicitor acting for haemophiliacs “did play-down the significance of hepatitis C” saying that it was “no big deal.”
In addition, the risks were significantly played down by haemophiliacs own consultants, whilst at the same time, government delayed the introduction of a hepatitis C test until months AFTER the signing of the hepatis waiver. As Matt Kelly QC points out:
At Paragraph 20 for example it is clearly pleaded that haemophiliacs were at great and particular risk of infection with Hepatitis B and/or NANB viruses and/or other viral infections from blood products used by them which, in the case of Hepatitis B and/or NANB could cause a serious illness of jaundice, liver disease and could sometimes lead to death, and in the case of other viral infections could cause serious illness and could lead to death. The same was pleaded in relation to the risks of commercial concentrates.”
Kelly concludes,
I have the greatest sympathy for Mr Longstaff. His life has, not to put too fine a point on it, been destroyed by the infected blood he was given. He was told by one of the key solicitors in the litigation not to worry about hepatitis C when it was plain that hepatitis C carried with it enormous risks and was a matter of grave concern.
The waiver was signed by all haemophiliacs in May 1991 and resulted in a paltry “out of court” settlement where government escaped public scrutiny of their blood policy documents and doctors and local health authorities avoided investigations into their treatment of haemophiliacs and families.
In the February 1991 aforementioned letter from Rejman, writing to others involved in the government side of the HIV litigation, he details the following in relation to Kernoff,
During a brief conversation with Dr Peter Kernoff, of the Royal Free Hospital, he mentioned to me that he has received a couple of writs in respect of hepatitis infection in haemophiliacs.
These are individuals that are HIV negative, and as such would not be covered by the HIV haemophilia settlement.
I believe that any that are HIV positive would have to agree not to raise hepatitis in any further litigation , but this obviously does not include those not in the scheme.
Dr Kernoff did not believe that the Department of Health was a named defendant at present, but I felt you would wish to be aware of this.
This author (who has seen much of the HIV litigation documents unredacted and knows how damning they are) notes it would not have been in the interests of the government or Dr Kernoff for haemophilia cases to go to court for either HIV or hepatitis C due to key evidence alleging liability based on a series of delays, withholding of key information/evidence and catastrophic failures relating to safety of treatment.
The launching of hepatitis cases where haemophiliacs did not have HIV coincided with the beginnings of the destruction of government documents and hospital medical records highlighted in media stories throughout the years following the HIV litigation. Haemophiliacs that did have HIV were then discovering for the first time that they had been tested often without permission for hepatitis C, had a positive result but had signed away their rights to litigate for hepatitis viruses. In order to take a case to court for alleged negligence, Grayson and Longstaff first had to challenge the waiver and to do so relied on being successful in accessing legal aid.
Their first point of call was to return to the solicitors that had represented them in the HIV litigation but increasingly a case was emerging that their own lawyers were allegedly implicated in holding back key evidence from their clients and had even lied about their chances of success of winning which they had later discovered were deemed far higher than they had been told in 1991. On that score, a note found in old litigation files read… “I can no longer lie to my clients” referring to an opinion that the chances of winning with regard to those infected from US factor concentrates had “significantly increased.”
What this author did find out was that in some cases, soon after 1991, the very same lawyers that had lied to HIV haemophiliacs were suddenly taking on cases of haemophiliacs with hepatitis C where they did not have HIV and had not signed a waiver. Incredibly they were also using the damning hepatitis evidence from the HIV litigation, never shown to HIV positive haemophiliacs at the time of their cases or before they signed the waiver. Although haemophilia hepatitis C cases were now being funded by legal aid, (so lawyers got paid)… they were never actually progressing the cases to be heard in court. Grayson and Longstaff had not one but 3 complaints upheld by the Office of Supervision of Solicitors against obstructive lawyers including allowing a case to deliberately go out of time.
A decade after the HIV litigation ended, Grayson teamed up with a haemophiliac named Peter Mossman co founder of the Manor House Group assisting lawyers with his case as well as supporting her husband’s waiver case. There were angry calls in writing from Mossman and other haemophiliacs to investigate one particular individual at the Legal Services Commission that was refusing to examine the HIV litigation evidence on hepatitis C and was alleged to be deliberately blocking cases, closing them down as legal aid certificates came to be renewed. I was later informed by a solicitor of the fact that government were notified of cases where they were the defendant by those deciding on whether legal aid should be granted… “forewarned is forearmed” as the saying goes. Haemophiliacs were concerned that this might be why their cases went on for many years without moving.
Some haemophiliacs such as Colette Wintle could not access legal aid at all, prevented from taking a case for hepatitis infection due to the fact that her husband worked and his income had to be taken into account.
One haemophilia legal case known to this author did however proceed and was WON though government denied knowledge of such cases when they received a Freedom of Information request from Grayson. This author spoke to the person involved at some length over a period of time following her case. Again this win demonstrated that had the evidence collected in the HIV litigation to support original litigants been presented in court in 1991, that there was a much stronger chance of haemophiliacs winning their cases than they were led to believe which should have been not only for HIV but also hepatitis viruses. Indeed the baseline arguement of the original litigation was that had more been done in relation to protecting haemophiliacs from hepatitis many would not have become infected with HIV. The decision to put factor concentrates onto the market first in the US before finding a way to virally inactivate was one of the worst and most dangerous decisions ever made regarding a treatment and hepatitis experts warned of this BEFORE factor concentrates hit the shelves for the first time.
In February 1996, this author wrote to Leonard Levy at the Department of Health in response to a letter received from him. she stated,
Many questions have still to be answered. Why did it take this country so long to utilize its own blood products? Why did this country use American blood products for so long when it was a well known fact that there were more contaminants in the American products. Was this an example of false economy for which many people have paid the price with their lives as a result of HIV and hepatitis C.
May I remind you of a recent case where the Plaintiff a carrier of the haemophilia gene won her case against the Health Authority, one of the main points being:-
“That the Health Authority administered to the Plaintiff American Factor VIII clotting factor which the Defendants, their servants or agents knew or ought to have known, was more likely to contain a hepatitis virus than English clotting agent which was already available.”
The Inquiry has been notified of the haemophilia hepatitis case that was won using the HIV litigation evidence but whether it will ever be examined is another matter as it would indeed open up a large can of worms in terms of how the original HIV litigation was handled, the many haemophilia hepatitis cases without HIV that then became “blocked” and which parties could be found liable. This author alleges this would likely be government, health authorities and some individual practitioners. (In America, the pharmaceutical companies did accept UK haemophilia cases that could demonstrate a certain level of proof, causality, tracing batch numbers to known infected prison donors for example) and cases are now closed in the US.
It is important to highlight also that although haemophiliacs were unable to take a case in the UK under the Product Liability Act for hepatitis C infection (as some whole blood cases did) as haemophiliacs infection occurred before a certain date, one aspect was very relevant to the HIV litigation. The BMJ highlighted that, Justice Burton ruled in 2001 that, “the NHS should have taken steps sooner to reduce the risk of transmitting the virus in blood and should have introduced screening by March 1990.”
Had this happened, haemophiliacs could have been tested with their informed consent BEFORE considering the waiver in 1991 and made an “informed” decision on whether or not to sign away their rights.
The Haemophilia community is tired of being abused and manipulated by government, their doctors and some past lawyers. Their message to all concerned is… “the game is up”! Long standing campaigners knew early on from the 1990s that relevant parties were conspiring to shut down legitimate legal cases. Interested parties destroyed documents, hid key evidence and blocked haemophiliacs every step of the way but families never gave up. Nor will they stop fighting until proper compensation is paid to haemophilia victims, partners and the bereaved. They should have received compensation 30 years ago for All viruses instead of facing delay after delay denying them a public inquiry and dirty tricks being played blocking the recommendations of the privately funded Archer Inquiry denying them compensation based on lies once again. They must also now be compensated for exposure to v CJD but that is another story that will be written by this author shortly. Campaigners have learnt never to put all their eggs in one basket. They are prepared as ever and will continuing fighting until they get what they deserve.
Carol Anne Grayson is an independent writer/researcher on global health/human rights/WOT and is Executive Producer of the Oscar nominated, Incident in New Baghdad. She was a Registered Mental Nurse with a Masters in Gender Culture and Development. Carol was awarded the ESRC, Michael Young Prize for Research 2009, and the COTT ‘Action = Life’ Human Rights Award’ for “upholding truth and justice”. She is also a survivor of US “collateral damage”
Journalist Shireen Abu Akleh who was brutally killed (Image credit to Al Jazeera)
Dear Nick,
As your constituent, I am writing to you to express my horror and revulsion at the shooting to death of Al Jazeera journalist Shireen Abu Akleh and the shocking and violent attack on mourners at her funeral by Israeli forces. This cannot be accepted and Israel must be held to account.
This is certainly not the first time a journalist has been targeted and Palestinians are subjected to multiple daily human rights violations, brutality, repeated detention including minors, confiscation and destruction of homes and land and restriction on the right to worship at Al- Aqsa mosque. Christians are not left untouched either.
So, I ask you to call for a ban on UK political groups calling themselves “Friends of Israel” whether left or right. How is it possible to remain friends with such an abusive regime?
I have campaigned long and hard to support the rights of Palestinians and as you are already aware, the rights of haemophiliacs given contaminated blood including my late husband and brother in law now deceased.
Recently I emailed Dame Diana Johnson MP (Labour Friends Of Israel) who is also Chair of the APPG for Haemophilia and Contaminated Blood raising my concerns regarding the medical apartheid treatment of Palestinian haemophiliacs, some also infected with deadly viruses. I had previously interviewed Jad K Jadallah Tawill, Founder and Board Director of the Palestinian Bleeding Disorders Community in the West Bank and Gaza Strip who painted a grim picture of the daily struggles of Palestinian haemophiliacs. I am including the following quote from Jad in a recent article from the Palestine Chronicle, March 12th, 2021 as follows:-
Right to Health is a Right to Palestinian Hemophiliacs Too
Quote,
Palestinian bleeding disorder patients and their families are a marginalized segment of the local community as well as the Middle East in general. They suffer extremely from the Israeli Occupation of Palestinian land as well as the geographical separation and movement restriction between the West Bank, the Gaza Strip, Jerusalem, and the outside world. These patients and their families are deprived of their human, medical, and social rights in addition to the violations they face from the Israeli military government rule.
I also drew attention to my concerns over the misuse of Israeli Pegasus spyware which is being sold around the world and used on NGOs, lawyers, journalists, politicians and campaigners and to recent legal cases launched including one in the UK by Bindmans.
Bindmans launches legal action in the United Kingdom on misuse of Pegasus spyware (19th April 2022)
To my horror, Dame Diana Johnson then e-mailed back saying she would not indulge in “nakedly anti-semitic conspiracy theories”. The above are stated fact NOT anti-semitic conspiracy theories. I am certainly not antisemitic. I have been invited to talk at Holocaust Memorial events, one event was attended by my former MP Jim Cousins, I have read many books on the holocaust, visited Auschwitz and other holocaust memorials across Europe and travelled with Jewish American friends across Asia.
I also note that despite sending Johnson my ESRC Michael Young awarded dissertation on Contaminated Blood at least 3 times, also sent 3 times by a campaign colleague Colette Wintle, she has failed to respond or act on the content which led to the withdrawal of the government’s only definitive report on Contaminated Blood. I question whether my public support for Palestinians has influenced her decision to ignore my findings? The report was the DOH Self-Sufficiency in Blood Products in England and Wales A Chronology from 1973 to 1991, which was withdrawn as a “whitewash” and as you know we finally now have the Infected Blood Inquiry to investigate how haemophiliacs came to be infected with HIV and hepatitis viruses chaired by Sir Brian Langstaff.
Given the long standing human rights violations by Israel which are growing by the day and the dreadful shooting of Shireen, I feel this cannot go without accountability and disbanding the Friends of Israel groups is one way of expressing strong disapproval from the UK. I am also deeply concerned at Keir Starmer’s seemingly unquestioning support for an apartheid state which to many left wing supporters means Labour has now become a party that no longer deserves our vote.
I am also increasingly disturbed by the false claims of “antisemitism” being labelled at anyone expressing support for Palestinians and Jews are among the worst affected. I abhor antisemitism and note legal cases are now being won against these fake claims which are only distracting away from genuine cases.
So in respect of the memory of Shireen and other journalists witnessed to have been killed by Israeli forces, respect to Jad K Jadallah Tawill and the many Palestinians denied their basic rights, respect to human rights activists now being spied upon and with respect to those falsely accused of antisemitism for supporting Palestinian rights, please call for a ban on political groups calling themselves, “Friends of Israel” an apartheid state. I refused to tolerate apartheid in South Africa and I won’t tolerate apartheid targeted at Palestinians.
I note also that the right of ordinary campaigners to express themselves is also under threat these days in the UK with growing restrictions on freedom of speech and the right to protest and now attempts to ban Boycott, Sanctions and Divestment (BDS) a peaceful and legitimate way to oppose apartheid Israel and occupation. It is not BDS we need to worry about but the negative influence of Israel on British politics left and right.
Evidence of Israel being an increasing aggressive and out of control apartheid state is backed by numerous reports from Amnesty International, Human Rights Watch, the UN, B’Tslem and respected educational institutions such as the Harvard Crimson Editorial Board.
I look forward to your prompt response.
(Full address supplied)
With thanks
Yours sincerely
Carol Grayson
Carol Anne Grayson is an independent writer/researcher on global health/human rights/WOT and is Executive Producer of the Oscar nominated, Incident in New Baghdad. She was a Registered Mental Nurse with a Masters in Gender Culture and Development. Carol was awarded the ESRC, Michael Young Prize for Research 2009, and the COTT ‘Action = Life’ Human Rights Award’ for “upholding truth and justice”. She is also a survivor of US “collateral damage”
Haemophiliac Peter Longstaff (deceased) shows the record cards that detail the US factor concentrate treatment that infected him with multiple viruses
A recent court of appeal dismissal rejecting permission to apply for a Judicial Review to examine whether the government funded English Infected Blood Support Scheme (EIBSS) acted in a discriminatory way has highlighted the importance of re examining haemophilia cases already registered with the scheme. EIBSS which was set up in 2017 provides financial and other support to those infected with HIV and/or hepatitis C through blood and blood products used by the NHS and to their families. There are similar schemes in Scotland, Wales and Northern Ireland.
UK Human Rights blog wrote on the case of CN v Secretary of State for Health and Social Care [2022] EWCA Civ 86 and quoted the following decision,
In a judgment handed down on 4 February 2022, the Court of Appeal dismissed an appeal for permission to apply for judicial review concerning the lawfulness of the England Infected Blood Support Scheme (EIBSS) (the “Scheme”). The Court of Appeal concluded that the Scheme’s exclusion of those infected with hepatitis B was not discriminatory. In any event, the Secretary of State’s justification for who was to be compensated under the ex gratia Scheme was to be given a wide margin of appreciation by the courts.
However it is important to note that the case in question with regard to the dismissal centred not on haemophiliacs that received a treatment called factor concentrates made from the pooled plasma of many thousands of donors (often from the US) but on the case of a person referred to as CN who received a whole blood transfusion within the UK. These were historically totally separate legal cases relying on very different evidence only recently pushed together in the Infected Blood Inquiry chaired by Sir Brian Langstaff. The legal case statement regarding CN which was released reads,
CN put the claim on the basis that there had been a refusal to include persons in his position within the EIBSS. CN suffers from hepatitis B virus (HBV) which he alleges he contracted when he was given blood transfusions on or after 14 April 1989, when he underwent a bone marrow transplant at Hammersmith Hospital. It is now accepted that the NHS screened blood and blood products for HBV at least from the mid-1970s.[3]
Unlike the unfortunate CN, infected haemophiliacs are ALREADY on the scheme in recognition of their HIV and hepatitis C infection which occurred in the 1970s and 1980s before viral inactivation and testing was put in place but the government has always refused to also include hepatitis B.
The recent dismissal of the whole blood case highlighted that,
“The eligibility criteria for support implemented by the Alliance House organisations were carried over to the EIBSS. [These] criteria [did] not include infection with hepatitis B because blood donors were screened for hepatitis B from 1972. There was therefore a significantly lower probability of blood being contaminated with hepatitis B in the 1980s than for HIV and hepatitis C, for which screening was introduced in 1985 and 1991 respectively”.
Although this statement may be applicable to cases such as that of CN with his whole blood transfusion, it is a complete nonsense where many haemophiliacs are concerned as it fails to address the fact that haemophiliacs not only received products manufactured using UK plasma but also treatment products manufactured in the US. It is important to note that evidence shows the collection procedures in the US during the 1970s and 80s violated almost every safety rule in the book including with regard to screening donors for hepatitis B.
The dangers of hepatitis B have long been known by UK authorities and were well recorded PRIOR to the importation of US factor concentrates in 1973. It was recognized in medical journals and by the UK government that plasma collected from remunerated donors on skid row and in Central America slum areas combined with plasma from drug users, prostitutes, gay men and prisoners in pools of up to 400,000 carried a far higher risk of transmitting hepatitis B than plasma sourced from the more carefully screened unpaid donors within the UK.
This dangerous imported treatment was even trialled on children with haemophilia at Lord Mayor Treloar College in Hampshire (a boarding school for children with disabilities) and is the subject of a newly launched legal case focusing on the alleged experimentation at the college. Before the introduction of US factor concentrates, haemophiliacs were treated with cryoprecipitate made from only a handful of volunteer donors thus keeping hepatitis infection to a minimum. Once US factor concentrates were introduced, former pupils recalled outbreaks of hepatitis B and being made to use plates in the canteen that were marked with a red dot to identify those infected.
As the Newcastle Journal “Bad Blood” campaign published in 2001,
DOCTORS were warned of the risks of using imported blood as early as the 1960s, a leading Newcastle scientist said last night.
Dr Arthur Codd, a consultant virologist in the Public Health Laboratory Service at Newcastle’s General Hospital, said he and others had warned about the risk of infection for many years.
“We had known that pooling blood from many donors increased the risk of contamination as early as the Second World War,” he said.
“Hepatitis B was transmitted to many people during this time and there was nothing we could do to prevent it.
“Crazy as it seems, a blood transfusion can seriously damage your health and our recommendations to only use blood from local donors were very clear.”
Until the UK started to import blood products from America, it had one of the lowest rates of hepatitis of anywhere in the world.
It is well documented by medical experts that haemophiliacs were infected with hepatitis B and non A non B (hepatitis C) from their first shot of commercial factor concentrates as the risks were so high.
To the editor- The probability of a recipient developing serum hepatitis (SH) is 10 to 50 times greater when the blood donor is a commercial donor. (JAMA, 24 th July, 1972, Vol 221. No 4)
Indeed as soon as commercial concentrates were introduced in the US, clusters of hepatitis B infections in American haemophiliacs were detailed in a 1972 study by Kasper and Kipnes who discussed their findings in the Journal of the American Medical Association in a letter entitled Hepatitis and ClottingFactor Concentrates, stating,
“Recent reports (listed 1-3 and referenced from 1970 and 1971) have aroused alarm about the danger of hepatitis after the infusion of clotting factor concentrates prepared from the pooled plasma of many donors. We have therefore reviewed the incidence of clinical hepatitis among 482 haemophiliacs treated here in the last 10 years (Reference to Table 1 in the article). The peak incidence occurred in 1968 in Haemophilia A and 1971 in Haemophilia B. Concentrate became the predominate mode of therapy in Haemophilia A in late 1967 and in haemophilia B in late 1969.”
They also warn later in the letter,
“We conclude that older children and adults who have had little exposure to blood products are at a high risk of developing clinical hepatitis after introduction of clotting factor concentrates. In such patients especially those with mild haemophilia, single donor products are preferable. On the other hand patients with severe haemophilia who have had many blood and plasma infusions have no increased risk of hepatitis if concentrates are used.”
However the American study did not take into account the effect on UK haemophiliacs (who did not start their imported treatment until 1973 in most cases) and the differences in collection practices and safety procedures between the UK and the US.
We now know that round 99% of haemophiliacs infected with HIV registered with EIBSS are co infected with hepatitis C and their medical records show most as having also been infected with hepatitis B, all impacting on the liver. Then there are haemophiliacs on EIBSS files without HIV but with hepatitis B and C. In addition to this haemophiliacs were re-infected over and over again further damaging their liver and immune system. Haemophilia is hereditary so you could also have (and often did) more than one family member infected. Some haemophiliacs also had the combination of hepatitis B and D as follows,
Hepatitis D is a serious liver infection caused by a virus that is transmitted through blood or bodily fluids. It can only be contracted if a person has had the hepatitis B virus and is uncommon in the United States. (Though not so uncommon in haemophiliacs.)
The case for haemophiliacs is very specific as a choice was made by government to introduce the recognized more dangerous imported factor concentrates BEFORE a way was developed to virally inactivate hepatitis B. Indeed this was well documented in the 1991 HIV litigation where it was argued that had government taken more action to limit hepatitis B exposure such as holding on from introducing factor concentrates until viral inactivation was in place and not importing US plasma, many lives could have been saved with regard to HIV and hepatitis C.
Safety should have come first even if it meant delaying putting the new so called “miracle” treatment on the shelves but governments and plasma companies put profit before safety and repeatedly turned a blind eye to safety violations. So the statement on “eligibility criteria” for EIBSS and the issue of hepatitis B infection sources and failures carefully avoids addressing the haemophilia cases where they received imported plasma. So far, despite many alleged safety violations related to hepatitis B the government has denied accountability for exposing haemophiliacs to a far higher risk of contracting hepatitis viruses from US treatment compared to the UK. This was particularly of concern given the far higher number of donors (many of them considered “high-risk”) in the American plasma pools.
Although the recent case dismissal was not successful for CN, it has certainly served to highlight the difference between haemophilia and whole blood cases in relation to hepatitis B infection and the importance of reviewing the two cases completely separately in terms of EIBSS.
The case highlighted that, as far as including hepatitis B within the EIBSS schemes,
Mr Tankel (for the defence) submitted that nothing has changed since 2004. HBV sufferers were not included then and they are not included now.
And there lies the shame, Tankel is absolutely right, to this day, the haemophilia cases have never been reviewed looking at the evidence which showed alleged negligence in the same way as the infections with HIV and hepatitis C. Tankel completely ignores the fact that former Health Minister Anne Milton removed the word “inadvertent” infection of haemophiliacs with HIV and hepatitis viruses in 2009 but the EIBSS scheme has so far failed to reflect that change and pay monthly support in recognition that haemophiliacs were also infected with hepatitis B. Exposure to v CJD is not included either.
In case Tankel is not aware, the original hepatitis payment scheme Skipton (which was scrapped and is now under EIBSS) was set up in the early 2000s to prevent haemophiliac Peter Longstaff going to court on his legal challenge to overturn the hepatitis Undertaking (waiver) in the 1991 HIV haemophilia ex-gratia settlement. A legal opinion from his then QC stated that it could not be “informed consent” as documents showed that everyone on the defence and those representing Longstaff, knew of the dangers of hepatitis viruses which they played down, keeping key evidence from Longstaff and others. Much of the HIV litigation documentation contained documents on hepatitis B and C which was seen by long standing campaigners following their own research and only some years AFTER the litigation ended in an out of court settlement withholding these important government and other papers.
Carol Grayson, Longstaff’s wife fought to legally access copies of papers that government had “inadvertently” destroyed from a solicitors office in Newcastle for her dissertation research awarded the Michael Young Prize. In response to a request from government, she returned copies in 2006 which were put onto a Department of Health website, then transferred to the National Archives Kew. However, this was not before the department lawyers had destroyed the legal letters of return through her instructions to solicitor Paul Saxon, Blackett, Hart and Pratt LLP and failed to reference Grayson as the provider. (Fortunately she retained her own copies.)
During the Archer Inquiry into contaminated blood which dealt ONLY with the infection of haemophiliacs, Lord Archer recommended haemophiliacs were paid out per virus and v CJD prion exposure. This should have been fully in place starting from 2010 but was blocked by the misinformation coming from Lord Warner. Compensation on a parity with Eire was blocked due to lies told by members of the British government regarding the Irish settlement. The Infected Blood Inquiry chaired by Sir Brian Langstaff have been asked to investigate this.
The UK Government continues to operate a “3 viruses for the price of 2” scheme to avoid accountability from the very beginning of the use of factor concentrates where there was almost non -existent safety screening in relation to hepatitis B in the US. This as mentioned formed a major part of the1991 HIV haemophilia litigation.
The question is… Was Tankel, the QC who represented government in the CN case commenting out of ignorance? Did he really have no understanding of the history of haemophilia infection compared to whole blood cases and safety issues over US treatment or is he carrying out more “damage limitation” for government so they can limit compensation payments? The Haemophilia Society represent haemophiliacs whilst the Hepatitis C Trust represents whole blood cases. Indeed, Charles Gore, former CEO of the Hepatitis C Trust recognized the differences between the 2 cases in writing within a journal article, evidence presented to the Infected Blood Inquiry.
It is important that whole blood cases do receive compensation but the facts surrounding infection are very different from haemophiliacs and there is no escaping the legally documented facts. Levels of payment should reflect multiple infections and EIBSS payments should reflect that.
The case for haemophiliacs receiving US plasma was always reported as the strongest case legally due to the fact for example that legal depositions highlighted that gay men were targeted for their “hepatitis B” rich plasma to be used in research …however the surplus was then added to top up the plasma pools for factor 8. Plasma wagons were in fact stationed outside the gay bath houses in San Francisco in the then notorious Tenderloin area specifically to bring in gay men for donation. From the early 1980s, hepatitis B came to be known as a warning sign for potential AIDS infection in the homosexual population. In addition to this, US prisoners who were administering the paperwork related to the plasma programmes at prisons such as Arkansas, falsified the names of inmate donors (known drug users) infected with hepatitis viruses and having unprotected sex (whilst waiting to donate) using names from a local telephone directory so they could sell their blood spreading infection with hepatitis B, C and then HIV. Thus infection of haemophiliacs was almost guaranteed with the use of commercial factor concentrates.
In some haemophiliacs you also had the combination of hepatitis B and D as follows,
Hepatitis D is a serious liver infection caused by a virus that is transmitted through blood or bodily fluids. It can only be contracted if a person has had the hepatitis B virus and is uncommon in the United States. (Though not so uncommon in haemophiliacs.)
It is clear that the recent dismissal case fails to understand the unique position of haemophiliacs living with hepatitis B, C, D and HIV all interacting with each other along with exposure to different competing genotypes, which can make treating haemophiliacs quite a challenge. This is very different to a one off infection from whole blood. Campaigners hope that Sir Brian Langstaff along with Sir Robert Frances also looking at compensation for Contaminated Blood victims will review hepatitis B infection in haemophiliacs in relation to EIBSS payments as well as compensation and end the government “bargain basement” style payment schemes for multiple viruses. If government wanted to avoid compensation payments, they should have done a far better job in protecting those now infected and affected through this scandal.
Carol Anne Grayson is an independent writer/researcher on global health/human rights/WOT and is Executive Producer of the Oscar nominated, Incident in New Baghdad. She was a Registered Mental Nurse with a Masters in Gender Culture and Development. Carol was awarded the ESRC, Michael Young Prize for Research 2009, and the COTT ‘Action = Life’ Human Rights Award’ for “upholding truth and justice”. She is also a survivor of US “collateral damage”
Wintle and Grayson (holding T shirts) join other Contaminated Blood campaigners in one of their many demonstrations outside the Department of Health, London
Late Friday afternoon on the 28th January 2022, core participants of the Infected Blood Inquiry which was set up in 2018 and is chaired by Sir Brian Langstaff received a notification via the Inquiry titled, Update on Sir Robert Francis compensation framework. This was a publication from the Cabinet Office and the Rt Hon Michael Ellis QC MP and highlighted that Francis had “published the notes of the six meetings he held in 2021 with groups of people infected and affected, and one meeting with legal representatives” see following link,
On reading the report, to say the author of this post was gobsmacked would be an understatement. It was immediately glaringly obvious that the Conference Call telephone meeting Carol Grayson and Colette Wintle both long standing haemophilia campaigners of over 3 decades held on the 10th December 2021 with Francis was not recorded in the update. The meeting was scheduled for 1 hour and was extended to around 1 hour 40 minutes with David Kirkham (Cabinet Office) also in attendance. However, the contributions of other groups (who appeared on the scene decades AFTER Grayson and Wintle began their activism) and newer groups’ proposals for a compensation scheme for those infected and affected by Contaminated Blood were recorded in some detail.
Following on from this revelation, it soon became apparent from talking to the Haemophilia Society, a national charity that represents those with inherited bleeding disorders whose lives were largely destroyed by what Lord Winston described as “the worst medical treatment disaster in the history of the NHS” were not included either. They were “dismayed” at this development. Haemophiliacs constitute a “distinct patient group” designated a “Special Status” by Virginia Bottomley at the time of the HIV litigation in 1991. They were infected with HIV and hepatitis viruses during the 1970s and 80s from factor concentrate treatment used to provide the missing clotting factors injected into their veins. Much of this treatment was imported from the US and made from huge plasma pools of up to 400,000 “high-risk” paid donors and violated virtually all of the safety rules of the day.
Grayson and Wintle then discovered that the Hepatitis C Trust that represent many victims infected by whole blood transfusions were also not included in the Cabinet Office update. In addition, they also learnt that at least 2 other long standing campaigners representing the haemophilia community and a further group representing non haemophiliacs that held their own separate meetings with Francis were not documented in the report either. So with the Grayson and Wintle meeting, it appears that 6 meetings are missing from the report, perhaps more?
It is important to note that it would have been inappropriate for Grayson and Wintle to attend meetings directly with other campaign groups due to a “conflict of interest” with some participants regarding alleged plagiarism of Grayson’s research and their fight to also ensure that the Special Status granted to haemophiliacs continues to be upheld. The Special Status criteria also extends to haemophiliacs with hepatitis C as well as HIV. As a result of these issues, Sir Brian Langstaff allowed the pair to be represented separately by Leeds firm, Milners and QC Sam Stein instead of by one of the four original legal firms appointed to the Inquiry.
For the two activists, exclusion of their comments and proposals on compensation in the Francis update echoes a long pattern of successive governments excluding long standing campaigners from key meetings and failing to minute the content over a substantial time period. The recent omissions are at best highly insensitive, at worst a continuation of the appalling “divide and conquer” tactics used over decades by senior civil servants and ministers dividing those infected by virus and pitting one haemophilia group against another.
This unethical behaviour has been catastrophic to the community causing splits within families where often more than one member lives with a bleeding disorder and is infected and affected. It has divided a group of patients who because of their condition and time spent in hospitals together with bleeds got to know each other very well. Haemophiliacs were traditionally, a tightly bound community in many ways who lives have been intertwined from the cradle to the grave. They boarded at special schools together which catered for their disabilities such as Lord Mayor Treloar in Hampshire, spent holidays and leisure time with one another in Haemophilia Society caravans, attended each others weddings and tragically said goodbye to their friends in each others company at the many funerals held for those who died as a result of their infections.
The following is one example of earlier exclusion where some haemophilia campaigners were treated differently to another….
Not long before the Infected Blood Inquiry was set up, long standing haemophilia campaigners were deliberately excluded from a key meeting with a government mediator to discuss the scrapping of the Macfarlane Trust and Skipton Fund along with other trusts. The government LIED saying all groups had been included in discussions and had been given an opportunity to comment. The reality was the exact opposite. When Grayson did a Freedom of Information request, her group Haemophilia Action UK (formerly Haemophilia North set up in 1994 and well known to government) was omitted from the official list of campaign groups. Other groups more recently formed were on the list. Then, Grayson and Wintle failed to receive a questionnaire devised to elicit opinions on getting rid of the Trusts until it was far too late to respond.
The irony was, Grayson, was the first female to represent partners (later widows) on the Macfarlane Trust Joint Partnership Group. She, Wintle and their friend the late Peter Mossman who founded the Manor House Group in the same year were never given an opportunity to raise concerns or objections regarding the obliteration of these Trusts. They have since taken their concerns to the Infected Blood Inquiry as to whether this action was even legal. Grayson had attended a meeting at the Macfarlane Trust years earlier where she was reassured that the Trust would remain for as long as the last infected and affected beneficiary remained alive. What happened to that commitment? Lawyers who represented haemophiliacs in the HIV litigation which led to the setting up of the Macfarlane Trust were never informed either that it was being closed down so were unable to advise their former clients of their rights if so required.
Even at the beginning of the Contaminated Blood Inquiry there was uproar at another exclusion when Catherine Nalty, Deputy Secretary to the Infected Blood Inquiry, took it upon herself to organize a meeting with then Health Minister Jackie Doyle-Price again leaving out the longest standing campaigners. She also allegedly breached confidentiality by putting two separate groups together in the same meeting whose cases were not comparable and whose infections were acquired through entirely different treatments. Grayson and Wintle have since refused to have any dealings with her due to a serious breakdown of trust.
So why do government and their cronies leave out long standing campaigners or fail to document and minute the content of meetings that have taken place including those with ministers?
Well one answer is this… The activists that have been around for decades know their Contaminated Blood history well, they have accumulated much valuable lived experience, have carried out their own awarded research into key issues, some have even worked in the field as HIV emerged and nursed those with blood borne viruses in hospital settings as well as caring for loved ones that were infected. They have sat on Trust groups, have files piled high to the ceiling of letters to government and the dismissive, dishonest and inadequate replies, discovered copies of thousands of blood policy documents government “inadvertently” destroyed, have participated in both litigation for their infections here and in the US and taken government to court in Judicial Reviews. In other words, they are knowledgeable, not naive and won’t have the wool pulled over their eyes by unscrupulous officials. That poses a potential threat to government who would rather sweep away their mistakes and alleged negligence under the carpet as indeed they have done for decades.
Back to Sir Robert Francis and current day concerns. Milners solicitors, the legal firm representing Grayson and Wintle were instructed to contact David Kirkham to express their discontent at the update exclusions and await to see whether details of their meeting and the content will now be included on the public record, transparency is essential.
It is important that ALL groups are treated EQUALLY. We expect the Haemophilia Society and other excluded groups will also be making representation if they have not done so already. The latest CEO, Kate Burt has shown herself to be a fast learner with regard to haemophilia history and has already gone a lot further in supporting the haemophilia community than many of her predecessors. Trustees such as Clive Smith, a haemophiliac with a legal background are now making important written contributions in the fight for justice for haemophiliacs.
Grayson and Wintle have long been public as campaigners, They put their heads above the parapet years ago facing the discrimination associated with AIDS and hepatitis and took the flak for those too afraid to speak up. Its not an issue for them that the general content of their meeting is made public, whether their names are included or kept confidential, they expect to be on the public record and given the same consideration and respect as other campaigners.
New campaigners have enthusiasm and determination no doubt which is to be applauded but much of their work has been rehashing old evidence by sending hundreds of FOIs to elicit evidence that original campaigners discovered. During her research, Grayson (whose work was awarded) ensured copies of many important government documents were placed in the public domain years ago. She organized for files to be placed on a Department of Health website and these were then transferred to the National Archives at Kew for others to access along with the thousands already saved by Grayson and the late Sir Patrick Jenkin who assisted her.
Long standing campaigners have been fighting for years, long before the Freedom of Information Act came into being, before the internet, emails, search engines and websites were a daily essential and before social media groups that has now made contact between campaigners so easy in locating one another. They ran awarded media campaigns from their own funds, not relying on others and without the special services of any London based Public Relations companies, it was all done through exhausting hard work. Government of course are well aware of this and would much rather deal with those that don’t have the extensive background when it comes to important Contaminated Blood issues, its called “damage limitation”. They will no doubt be looking for the cheapest possible options for future compensation as they did with previous “ex-gratia” payments. The “new kids on the block” are unfortunately far easier to manipulate than the older generation of campaigners, long toughened up by their years of painful experience, loss and hardship who will not be taken for a ride!
Carol Anne Grayson is an independent writer/researcher on global health/human rights/WOT and is Executive Producer of the Oscar nominated, Incident in New Baghdad. She was a Registered Mental Nurse with a Masters in Gender Culture and Development. Carol was awarded the ESRC, Michael Young Prize for Research 2009, and the COTT ‘Action = Life’ Human Rights Award’ for “upholding truth and justice”. She is also a survivor of US “collateral damage”.
Long standinghaemophilia campaigner Peter Mossman who was infected with hepatitis C following treatment with factor concentrates
Tribute written by his friends and fellow campaigners Colette Wintle and Carol Grayson
It is with great sadness, but equally an honour too, that we, Colette Wintle and Carol Grayson jointly write this tribute to our dear friend Peter Mossman, affectionately known as “Mossie” who died on Friday 17th of December 2021 at the age of 78 after a long battle with hepatitis C and other associated conditions. Peter was a member of the Haemophilia Society and a long- standing campaigner who fought tirelessly for a public inquiry into the tragic circumstances which led to the “worst treatment disaster in the history of the NHS” a shocking scandal of which he was a victim. He was brave, stoical, funny and a true friend who supported us through the many difficult times we experienced over the years and will be remembered with great fondness.
Peter’s greatest achievement was founding the Manor House campaign group in 1994, along with his friend the late Peter Hughes who was co-infected with HIV/Hep C. The ribbon emblem of red, yellow and black that so many people wear today, to represent the HIV/ HEPATITIS C haemophilia victims, was created by Peter’s campaign group, getting MP’s of all political parties to wear the ribbon in support of their constituents at the many debates and campaign gatherings we attended at Westminster and beyond. For many of the younger generations of haemophiliacs who are not aware of the campaign history, it must be realised that in the 1990’s there were no dedicated groups of campaigners challenging the government on the issues of Hepatitis C infection. It was a very difficult task at a time when there was huge stigma and fear over HIV and Hepatitis C, and so few of us who were willing to risk being openly public.
Sadly, the UK government were responsible for creating harmful divisions within the haemophilia community by failing to acknowledge Hepatitis viruses in the same way as HIV. This was reflected in the setting up of a support scheme through the Macfarlane Trust following litigation in 1991 for 1252 HIV infected haemophiliacs whilst at the same time denying those infected with hepatitis C much needed financial support until the formation of the Skipton Fund in 2004. This came about only after prolonged and relentless activism by Peter and other long standing campaigners and the establishment of a legal case to try to overturn a controversial hepatitis “waiver” written into the HIV litigation. The threat of going to court finally motivated government to act. Around 5000 haemophiliacs were infected in total with HIV and hepatitis viruses.
The divisions by virus were grossly unfair and ironic given that 99% of haemophiliacs with HIV also had hepatitis C. Peter refused to be drawn into such political games and in 1994 travelled from Manchester to Newcastle to meet fellow campaigner, the late Peter Longstaff who was infected with HIV and hepatitis C to forge a campaign strategy that would incorporate all haemophiliacs and their families. Both were also active in highlighting the exposure of haemophiliacs to variant CJD and vocal in their support for carers and bereaved families.
Peter, like many campaigners, was very unhappy that little was being done by official bodies to acknowledge the level of harm and damage caused by Hepatitis viruses, so his involvement and hard work in creating The Manor House Group helped to raise the profile of this terrible disease campaigning for better treatment and assessments for liver transplants which were still a rarity for haemophiliacs in the 1990s.
He actively worked with the media, contributed to documentaries and engaged the political support of his MP, the late Lord Alf Morris of Manchester (President of the Haemophilia Society for many years) as well as the late Paul Goggins MP. Peter worked hard to educate Paul on the history of the Contaminated Blood scandal, Paul in turn was instrumental in educating (then) Sec State for Health, Andy Burnham and “turning him around” (as Andy has acknowledged) to become an active advocate for the haemophilia community.
Pete was one of the first UK haemophiliacs to obtain legal aid in 1989 to fight for proper compensation for his hepatitis infection. He worked tirelessly with at least 5 firms of solicitors over many years trying to get his case to court. Carol often accompanied him to Chambers to consult with his legal team and present new evidence but the case was viewed as a “hot potato” that some lawyers were keen to let drop. Sadly after constant battles over maintaining legal aid the case was discontinued much to Peter’s anger and despair. When the files were reviewed at a later date as a new firm took over the archived documents, it was stated that Peter actually had a good chance of winning his case though it had not been allowed to proceed. Another great injustice which caused personal heartache for our friend. Tragically by the time Peter got Milners a good legal firm to represent him at the Infected Blood Inquiry alongside respected QC Sam Stein it was too late for Peter to assist in person due to declining health… the years of fighting for justice had taken its toll.
Peter, alongside a small number of us, were the early activists that despite the decades that came to pass, never lost hope that truth, justice and compensation would be achieved and helped build the platform of campaigning which many recognise and build upon today. He joined us in the early 2000s to file a complaint to the Dyfed Powys police which included allegations of corporate crime/manslaughter, alongside unethical experimentation and trials on haemophiliacs against the Nuremberg Code, without “informed consent, testing without permission, withholding positive test results, and numerous other key issues. He also submitted a complaint to the General Medical Council and met with our American lawyers representing haemophiliacs taking a case against the pharmaceutical companies in the US.
Mossie’s dedication to the cause has benefited many haemophiliacs within our community over the years and inspired a new generation of campaigners to add their contribution to what he helped establish. We give thanks to Peter and value his large volume of painstaking work and the happiness he brought his fellow campaigners along the way and send our condolences and love to his family and many friends near and far.
Carol Anne Grayson is an independent writer/researcher on global health/human rights/WOT and is Executive Producer of the Oscar nominated, Incident in New Baghdad. She was a Registered Mental Nurse with a Masters in Gender Culture and Development. Carol was awarded the ESRC, Michael Young Prize for Research 2009, and the COTT ‘Action = Life’ Human Rights Award’ for “upholding truth and justice”. She is also a survivor of US “collateral damage”.
HaemophiliacPeter Longstaff top row, second from the right was the subject of alleged experimentation at Treloar College in the early 1970s
In the year 2000, Peter Longstaff and his partner Carol Anne Grayson who set up campaign group Haemophilia Action UK made complaints to their local police in Newcastle, northern England, regarding a number of allegations in relation to Pete and his younger brother Stephen becoming infected with HIV and hepatitis viruses. Haemophiliacs are victims of what is now known as the Contaminated Blood scandal, which Lord Winston described as “the worst medical treatment disaster in the history of the NHS.” Some of the allegations related to medical treatment received as part of unethical trials whilst the boys were pupils at Lord Mayor Treloar College in Hampshire, a boarding school for children with disabilities. This scandal is now the subject of the biggest ever public inquiry in the UK known as the Infected Blood Inquiry which commenced in 2017 and is chaired by Sir Brian Langstaff.
Both Pete and Stephen had an inherited condition named haemophilia where the blood does not clot properly. In the early 1970s, whilst a pupil at Treloars, Pete who had previously been prescribed a treatment called cryoprecipitate manufactured using blood collected from a handful of UK volunteer donors was transferred over onto a new so called “miracle” treatment called factor concentrates, much of it imported from the US. However, the parents of children who were put on the first official treatment trials at Treloars in 1973 were never told of the greatly increased risk to their children and that hepatitis infection was almost 100% guaranteed from the first injection of US factor concentrates.
What they didn’t know also in the early1970s, was that the pharmaceutical companies that made the American products from pooled plasma relied heavily on “high-risk” paid donors such as prisoners, prostitutes, gay men and skid-row drug addicts. Plasma was also sourced from the island of Haiti and several Central American countries putting patients at risk from deadly viruses including those not prevalent in the UK. As well as viral risks to haemophiliacs, donors who were often from lower socio-economic groups that sold their blood were over bled thus depleting their health also.
In more recent times, the UK government has admitted to Grayson in a written answer to a Freedom of Information request that no risk assessment was ever carried out prior to importation of US products and the use of factor concentrates in 1973.
In a letter to Mr and Mrs Alice Longstaff dated, 12th April 1973, Consultant Haematologist, Dr Peter Jones, Newcastle wrote encouraging them to agree to Pete being put on the first UK factor concentrate trials at Treloars stating, that the treatment “could do nothing but good for the boys and other patients” but there was no mention of any risks. Old treatment records also show Pete had already received some factor concentrates in 1972 even before official licensing in 1973 possibly on a named patient basis. Grayson has still to obtain and go through records belonging to Stephen to investigate what treatment he received at Treloars.
The first complaint made to Newcastle police by Grayson and Longstaff was not taken seriously. So after a campaign rally in 2001 at Westminster, the couple along with fellow campaigners Colette and Steve Wintle went to the Metropolitan police to lodge a complaint there. The Met referred complainants back to regional constabularies. They then decided to embark on a co-ordinated complaint to regional police across England, Scotland and Wales during approximately the same time period, each taking their own evidence regarding individual cases. Local forces then referred campaigners to Dyfed Powys police in Wales that had a specific remit regarding “corporate manslaughter”. Again part of the complaint was the alleged experimentation on haemophiliacs used as “guinea pigs” at Treloar College and in some haemophilia centres. The issue of experimentation was also the subject of written complaints to the General Medical Council (GMC) AVMA (Action against Medical Accidents) the Department of Health and to human rights organizations including Amnesty International, Human Rights Watch and Liberty.
Years later, Grayson was told Dyfed Powys police investigation under controversial Chief Constable Terrence Grange (who later resigned following a series of allegations) was sat on and the evidence submitted by campaigners meant as a starting point was never followed up or expanded upon. In addition, many key persons, alive at that time (now deceased) that could have assisted with further evidence were never interviewed. The case was closed by the Crown Prosecution Service.
Last year, a virtual police conference took place at Cumberland Lodge which was set up as a form of reconciliation where complainants had been failed by the police in historic cases and included victims of the Contaminated Blood and Hillsborough football stadium scandals among others. Things did not get off to a good start. The first mistake the police made was the failure to identify the original long standing campaigners who had submitted complaints 20 years earlier, instead focusing on a new campaigner Jason Evans (the son of a haemophiliac) who was not involved in any way, shape or form with the original police complaint and only appeared on the campaign scene in 2017.
Grayson did have email contact with Rob Beckley, Assistant Commissioner of Operation Resolve who apologised but after some consideration she declined to participate as for her the issue of experimentation at Treloars is still very much active with the Infected Blood Inquiry. Grayson is requesting via her solicitors Milners of Leeds and Sam Stein QC that they make representation to the Inquiry that both Dyfed Powys police and the GMC are brought before the Inquiry barristers to be questioned on why complaints were not fully acted upon. Colette Wintle did participate and contribute to the conference but was not a pupil at Treloars. A report from this conference is due to be released on 1st February 2022.
Back on the 26th September 2018, the Northern Echo reported the opening statement of Sam Stein QC who represents Grayson (whose husband died in 2005) and the Wintle family highlighting that,
ANYONE who knowingly supplied contaminated blood to a patient who subsequently died is guilty of murder and should be prosecuted, an inquiry has been told.
Sam Stein QC, appearing at the infected blood inquiry on behalf of North-East widow and campaigner Carol Grayson, also said there had been a “systematic attempt to destroy evidence” of the scandal.
In June 2021, the Guardian reported on the case of haemophiliac Gary Webster infected with both HIV and hepatitis C who claims he was not aware of being part of a trial at Treloars stating,
“I honestly don’t remember having any information about going on trials research or anything like that. My parents never were informed of any of it … We always saw we were in some sort of weird experiment because we just couldn’t understand why they were pushing us so much to have all these injections.
It was also reported that “an undated consent form purportedly signed by his mother was shown to the inquiry but Webster said she had no recollection of it.” The paper also highlighted that,
Earlier, the inquiry in central London was shown a document that said Dr Antony Aronstam, the director of the haemophilia centre, “emphasised the necessity for research as the concentration of haemophiliacs found at Treloar’s is unique within Britain”.
On the 20th October, 2021 the BBC reported that Webster “has begun the first legal action by a former pupil against a Hampshire school where boys were given infected blood products” however complaints about unethical experimentation at Treloars to the police preceded Webster’s legal case by 2 decades.
Solicitor Des Collins acting for Webster stated, “There was a total failure to inform and obtain consent on the risks associated with the blood products administered and a deplorable dereliction of duty in the handling of his subsequent diagnosis.”
Old minutes and research papers discovered years ago by Grayson and part of the 1991 HIV Haemophilia litigation showed there that some studies relied on pupils at Treloars to participate in trials and that haematologists in local treatment centres across the UK co operated with doctors at the college and with researchers such as Dr Craske in finding subjects for alleged unethical experimentation. Patients were being quietly observed in treatment trials sometimes for years, in the case of Longstaff from his days at Treloars in the early 1970s right up to the beginning of 1990s without his knowledge or expressed permission and without “informed consent”.
When Grayson raised the general issue of “informed consent” in a letter to Dr Charles Hay (United Kingdom Haemophilia Centre Directors Organization, UKHCDO) in 2003, in an effort to obtain medical records and further information, he wrote back to her directly stating,
“I think it is completely misguided of you to stir up complaints to the General Medical Council. I cannot see this will achieve anything constructive and it can hardly be calculated to encourage support from the medical community for your campaign.”
He added,
“Unless you report the history of this tragedy in a balanced and straightforward way, DOH is unlikely to take your campaign seriously and you will not enjoy the support of the medical profession.“
After Grayson wrote to Hay about haemophiliacs being tested for hepatitis C without permission following infection via factor concentrates and their positive test results withheld sometimes for years, Hay responded to an email from Charles Lister at the Department of Health, who was inquiring about patients concerns stating,
“Most of the complainants belong to that impossible group of troublemakers, “Haemophilia Action UK” who would have some difficulty recognising the truth if it hit them in the face. They want money. The Haemophilia Society rightly regard them as a liability because their arguements are so unbalanced and they are so ready to lie that they lose all credibility. “
Since then many haemophiliacs in addition to Grayson and Longstaff have submitted evidence on testing without permission and withholding of positive test results which are now accepted as fact by the Infected Blood Inquiry.
Grayson went on to win two awards for her research on Contaminated Blood… The ESRC Michael Young Prize and the COTT Action = Life award with her husband for upholding truth and justice.
Returning to Treloars, over 72 former haemophiliac pupils have since died from their infections including both Peter and Stephen Longstaff. Over 3,000 haemophiliacs have died in total with many others harmed by their treatment. It is not only a scandal of how many haemophiliacs were used as guinea pigs and infected with deadly viruses but the appalling way they and their families were treated afterwards in their search for truth and fighting for justice.
Carol Anne Grayson is an independent writer/researcher on global health/human rights/WOT and is Executive Producer of the Oscar nominated, Incident in New Baghdad. She was a Registered Mental Nurse with a Masters in Gender Culture and Development. Carol was awarded the ESRC, Michael Young Prize for Research 2009, and the COTT ‘Action = Life’ Human Rights Award’ for “upholding truth and justice”. She is also a survivor of US “collateral damage”.
Arkansas prison plasma donor the late Bud Tant a known drug user infected with hepatitis C who was allowed to sell his plasma which was put into US pools of up to 400,000 donors
(Image, thanks to Linda Miller)
In the early 1970s when US factor concentrates were first licensed for introduction into the UK, haemophiliacs that have an inherited bleeding disorder where the blood has difficulty clotting, went from receiving cryoprecipitate, a treatment made from a handful of unpaid British donors to imported factor concentrates manufactured from plasma pools in America that over the years could reach as high as hundreds of thousands of paid donors. Many of these US donors were considered “high risk” for transmitting viral infections such as hepatitis B and included prisoners, drug addicts, prostitutes, skid -row donors, gay men and plasma sourced from donors in Haiti and Central American mainland countries.
As well as being high-risk for viruses, US prisoners for example were also the subject of unethical experimentation put on chemical trials with new drugs tested out on them, applied with new topical treatments that could affect the body through the skin, and injected with viruses which were sometimes deliberately mutated. These prisoners were STILL allowed to sell their blood, despite such experimentation resulting in a poorer quality of plasma and often unsafe donations.
Stanford Children’s Health describes plasma as “the largest part of your blood. It, makes up more than half (about 55%) of its overall content. When separated from the rest of the blood, plasma is a light yellow liquid. Plasma carries water, salts and enzymes.” It also contains clotting factors (which were used to treat haemophiliacs) as well as other components such as antibodies and the proteins albumin and fibrinogen. Haemophiliacs could be classed as mild, moderate or severe depending on the ability of their blood to clot.
A Freedom of Information request response recently received by long term campaigner Carol Grayson (Haemophilia Action UK) highlighted that no risk assessment was ever officially carried out by the UK government PRIOR to importing the so called “miracle” factor concentrate” treatment in 1973 This was particularly disturbing as the risks of pooling plasma had been written about for decades in international medical journals. Factor concentrates were small bottles of dried plasma that had to be mixed with sterile water and then injected directly into a vein.
Grayson has long argued that factor concentrates should never have been put on the market in the 1960 without first finding a way to inactivate viruses within the blood, even if this meant delaying the new treatment by several years.
As Grayson highlighted in a previous article on blood safety, as soon as factor concentrates were released onto the US market place there were outbreaks of hepatitis in the American haemophilia population. Jessica H Lewis wrote in Vox Sanguinus in 1970,
“The widespread therapeutic use of fractions prepared from large pools of plasma has increased the risk of exposure to SH (serum hepatitis) and has produced an apparent sharp increase in the incidence of jaundice (table 1 shown) in a group of 300 haemophiliacs seen in this clinic….”
Grayson’s husband, Peter Longstaff, a haemophiliac with less than 1% clotting factor who was treated with cryoprecipitate during his childhood years did not become infected with hepatitis until given his first US factor concentrates.
The Infected Blood Inquiry set up in 2017 to examine how haemophiliacs came to be infected with blood borne viruses chaired by Sr Brian Langstaff has been asked by campaigners to investigate pool size, historic and current and the associated risk of viral infection. (Those infected by whole blood transfusions are also included in the Inquiry, but they were NOT exposed to high plasma pools, NOT given blood from paid donors and NOT treated with imported blood.)
Haemophiliacs, on the contrary, have long been referred to as the “canaries in the coal mine”. In 2006, an ABC, Nightline article looking at the historic infection of haemophiliacs with HIV and hepatitis viruses had this to say,
Think of them as “canaries in the coal mine.” Like the fragile birds sent down into the mines to detect the first whiffs of toxic gas, hemophiliacs represent a first line of defense against any infectious threat to the nation’s blood supply.
If groups of hemophiliacs suddenly become sick, their misfortune may very well alert the rest of us to the dangers of bad blood.
For hemophiliacs, regular infusions of a blood-clotting agent made from donated plasma have become essential to life. This agent, known as Factor VIII, reduces their blood-clotting time from hours to just minutes. It has been received by hemophiliacs and their families as a miracle drug that permits children to play without fear of uncontrolled bleeding from a simple scrape and allows adults to live twice as long as they might have a generation ago.
But Factor VIII, which was synthesized from the plasma of 20,000 to 100,000 donors, also carried a significant downside: If one of these donors is infected with a blood-born virus, the miraculous factor would also be contaminated. Many hemophiliacs were exposed to the hepatitis virus in the 1970s and to AIDS in the early 1980s — experiences that suggest how a miracle can become a nightmare.
It wasn’t as if haemophiliacs were warned of the increased risks of going from cryoprecipitate to factor concentrates or the paid donors being used in imported treatment. Grayson’s late husband who attended Lord Mayor Treloar College in Hampshire as a child had his first US factor concentrates whilst on treatment trials. The boarding school catered for children with a range of disabilities including bleeding disorders. Peter’s parents received a letter from Newcastle Consultant Dr Peter Jones, who wrote to them on the 12th April 1973, stating,
You will have received a letter from Lord Mayor Treloar asking for your permission for Peter to participate in a special trial of regular factor VIII injections. The …… (referring to another child’sparents, name removed) have also been asked for their permission. I saw the …… last week and explained that I was in complete agreement with the trial and that it could do nothing but good for the boys and other patients.
It is important to note, that without knowing both the positives of taking treatment AND the risks, there is no “informed consent” which was deemed so important in the 1949 Nuremberg Code that produced key principles in terms of medical ethics.
Keeping in mind, some haemophiliacs were on prophylaxis treatment with factor concentrates three times a week to prevent bleeds and then extra treatment if they had breakthrough bleeds, you do the maths regarding how many hundreds of thousands of donors patients were exposed to potentially with each injection. This is why some doctors made efforts to ensure patients had treatment from the same manufacture with batch number in succession to avoid mixing factor concentrates and further increasing donor numbers but this was not always possible.
It is widely accepted that haemophiliacs were infected with hepatitis viruses B and C from their very first shot of imported commercial factor concentrates. Then they were often re-infected with different genotypes. It is also important to note that as haemophilia is an inherited condition there may be several family members born with haemophilia, receiving treatment and living with blood borne viruses.
Many years after the introduction of US factor concentrates to the UK, Corey Dubin, an haemophilia activist from the Committee of Ten Thousand (COTT) in the US highlighted the following regarding pool size that haemophiliacs were exposed to and in a video talk to university students, he said,
For years we were told that those pools were 30,000 donors per pool what we learned in internal industry documents was that those pools were anywhere from 30,000 donors to 300,000 donors which is a very different risk landscape, only the community never understood that.
UK haemophiliacs began to understand and question as they learned of the implications of their own infection with HIV and hepatitis viruses and watched their fellow haemophiliacs die. Acquiring knowledge was not made easy for the haemophilia community who were often tested for these viruses without their knowledge and permission using blood samples taken to check their clotting levels and then positive test results were sometimes withheld for years.
So what efforts were made to reduce pool sizes over the years and limit the spread of blood borne infections? It appears once heat treatment was introduced in the mid 1980s as a form of viral inactivation for factor concentrates, largely as a response to the emerging AIDS epidemic, little emphasis was put on limiting the number of donors per pool as a safety factor. This element was largely put on the back burner for another decade.
In 1996, a study in a September edition of Transfusion stated that, “risk of exposure increases with pool size and the prevalence of the agent in question and accumulates with repeated treatments with material manufactured from different pools.” The study also highlighted that, “reducing pool size would at best decrease this risk in proportion to the reduction in manufacturing scale. However, for individuals requiring repeated or continuous treatments, the risk of exposure to all but the rarest infectious agents would be only minimally affected, even by large reductions in manufacturing scale.”
Again this highlights why it was so important to put viral inactivation and safety first with factor concentrates not years later as a reaction to AIDS after the horse had already bolted.
Regarding receiving treatment from different pools… Longstaff’s records showed he had regular treatment from ALL the US plasma companies during the critical period of infection PRIOR to heat treatment and AFTER. It is no coincidence that the Newcastle Haemophilia Centre was noted to have the highest haemophilia death rates in the UK.
As previously mentioned, US pool sizes made with plasma from paid donors were considerably higher than those in the UK that used unpaid donors. Longstaff’s treatment was a mix of the 4 main US plasma company products with a much smaller amount of UK products. Depending on what was in the fridge at the haemophilia centre or at home, he could have different treatments with different products from different US pools even within the same day when on prophylaxis treatment or during an intense treatment period of several days if bleeding. A book written by Simon Garfield “The End of Innocence: Britain in the Time of AIDS” which included a chapter on UK haemophiliacs infected with HIV actually had a chapter titled, “the fridge that day” for that very reason.
Longstaff’s HIV infection was traced back to source with the help of lawyers and a documentary film maker Kelly Duda to an identified US Arkansas prison plasma donor via treatment batch numbers, a fact accepted by the US pharmaceutical companies involved in litigation. This prison plasma programme did not close down until 1991 which was years AFTER the UK stopped collecting blood from inmates, thus prolonging exposure to high-risk donors.
To reiterate, Longstaff had almost everything going in terms of different treatments manufactured from multiple high -risk, large donor number, plasma pools that included plasma collection that went against WHO guidelines with Longstaff receiving the aforementioned paid donations from Haiti, Central American mainland countries, US skid row donors, prisoners, prostitutes, drug users and gay men.
For those severe haemophiliacs that needed regular treatment and higher amounts over longer periods for bleeds it was especially important not to mix different treatments and different pools. Imported treatment from the US that relied on plasma from Central American countries also ran the risk of including viruses other than HIV and hepatitis viruses which were not generally present in UK donors or products. Donors were also over bled compared to the UK putting them at risk and sometimes to the point of collapse, this over bleeding depleted the blood of key elements and was again affecting the quality of the plasma.
Haemophiliacs who relied on only UK products were not exposed to the same level of mixing of different plasma pools as those who had predominately US products from numerous different companies and manufacturers with a far higher number of (remunerated) donors to the plasma pools.
On 31st July 1997, at at time when UK haemophiliacs were still being treated with American factor concentrates, a Congressional Hearing finally took place in the US titled, FDA Oversight: Blood Safety And The Implications Of Pool Sizes In The Manufacture Of Plasma Derivatives. The following is taken from that hearing with an introduction by Mr Christopher Shays, Chairman of the Sub Committee of Human Resources:-
Mr. Shays. I would like to call this hearing to order.
Welcome to our witnesses and our guests. To minimize the
risk of injury or death in the event of an emergency, the fire
safety laws set a maximum on the number of people allowed in
this room.
This was not a good way to open.
Surprisingly, the blood safety laws don’t contain the same
type of common-sense safeguard. There are currently no limits
on the number of blood plasma donations combined into the pools
from which therapeutic proteins are extracted or fractionated.
In the event of an emergency such as the appearance of a new
blood-borne infectious agent, excessively large plasma pools
increase the risk of disease transmission to the users of
plasma-derived products, and make recalls more difficult.
A user of a single dose of a fractionated product today may
be exposed to plasma from as many as 400,000 donors. Pool sizes
vary widely from company to company, product to product, lot to
lot, dose to dose. There is no standard.
Patients are not routinely informed of the risks associated
with plasma pool sizes. Last year, in our oversight report on
blood safety, we recommended, among other steps, that plasma
fractionators should limit the size of plasma pools, with pool
sizes determined as much by public health risk factors as by
production economies of scale.
Today, we ask Federal public health agencies, blood product
consumers, and the plasma industry what progress has been made
bringing safety considerations to bear and setting practical
upper limits on plasma pool sizes. For some products, pooling
is beneficial, even required, to capture a broad range of
antibodies, for example, or to extract a sufficient volume of a
scarce protein. For other products, however, there is an
undeniable and direct relationship between the number of donors
in the plasma pool and the risk of exposure to an undetected
infectious agent.
Tragedy taught us that lesson. In the early 1980’s, new
hepatitis strains and the human immunodeficiency virus, HIV,
slipped into the blood supply. Thousands died. Hundreds of
thousands were exposed to Hepatitis C, many of whom have never
been told of their possible infection.
Now other viral agents, and perhaps prion diseases, pose
similar threats to the safety of the blood supply. Yet the
risks presented by pool sizes have not been addressed.
A discussion on the issue of pool size included the following verbal exchange between Mr Shays, and a Ms Zoon, Ph.D, Director , Center for Biologics, Evaluation and Research, Food and Drug Administration
Mr. Shays. Is it fair to say the FDA was thinking that
these pool sizes were more like 10,000 and then learned it was
60,000? But wouldn’t it be pretty surprising for you all to
have learned that it was 400,000 in one instance? I mean, was
that a surprise?
Ms. Zoon. I think the number of 400,000 was high. I think
at the Blood Products Advisory Committee earlier, I believe a
presentation was made by one of the blood associations, that it
was potentially as high as 100,000. But 400,000, I think was
higher than I would have predicted.
Mr. Shays. Does that give the FDA a greater interest in
trying to take a look at this issue?
Ms. Zoon. Well, we are committed to putting a limit on pool
size.
Mr. Shays. OK.
Ms. Zoon. And I think as we get additional information and
analyze it and verify that information, we will certainly view
limits on pool size as part of a–our recommendations.
In the mid 1990s, the emergence of v CJD in the blood supply in some countries (which is a prion that can’t be killed in the same way as HIV and hepatitis viruses) appears to have been a big motivator for finally looking at limiting pool size following decades of mostly inactivity.
In 2005, pool size and safety continued to appear on the agenda, The Atlantic quoted the following, again highlighting that US plasma pools were significantly higher than those in Europe.
Critics today still question the wisdom of cutting costs by maintaining massive plasma pools. Safer systems operate on a not-for-profit basis, and require only sufficient amounts of plasma to meet domestic needs. A 2005 report published by writers at Ghent University in Belgium says that in Belgium, “approximately 5,000 donations are mixed into such pools. In Germany, pools containing up to 60,000 donations are considered.” In the United States, “some donor pool sizes are in excess of several hundred thousand [donations].”
So far, the Infected Blood Inquiry has only discussed evidence where US pool sizes reached 60,000 and it is important that further research is carried out to include documents detailing the far higher pool sizes that we now know existed and may continue to exist. Fortunately in 2022, most UK haemophiliacs are now on a product called Recombinant, a synthetic clotting treatment to treat bleeds However, this may not be suitable for all, leaving some patients still relying on human plasma products which have continued to be imported due to the risk of variant CJD in the plasma of UK blood donors.
As mentioned at the beginning of this article, for decades the UK has only collected blood from volunteer donors compared to the US that largely relies on the higher risk paid donors. World Health Organization 1975 guidelines highlighted the importance of countries being self-sufficient in their own blood products and not relying on remunerated donors. The UK failed miserable on the self sufficiency aspect but remained committed to not paying donors for their blood. A recent look at the blood.co.uk website which provides information on donation and collection to the general public, states the following,
In some other countries, plasma derived medicinal products are made from plasma donated by donors who are paid. These medicines can be imported to the UK.
It’s illegal to pay blood donors in the UK.
Seeing the world “illegal” came as something as a surprise. Illegal is defined as, “contrary or forbidden by law, especially criminal law”. (What would be the implications and penalties for a company/organization if they were to use blood from paid donors in the UK?)
The Adam Smith Institute blog, titled “Paying The Blood Price Is The Way To End Donor Shortages” (22nd August, 2013) also states,
The real issue is that it is illegal to pay for blood directly from the source but it’s not illegal to buy it from countries that have a surplus. Often this surplus is from paying their citizens to donate – like in the United States for example.
Over the years, the type of language used in publications regarding selling blood in the UK has tended to be along the lines of “against guidelines” “not permitted” “against the rules” “immoral” “high-risk” but not stated as “illegal” I have now written to both the website and the Department of Health and Social Care to ask them to clarify the following:-
Please can you advise,
What year was this ruling first introduced?
Under which part of UK legislation can I find this ruling?
Could you please provide a link.
It will be interesting to see how they respond. The point is however is that there is a great hypocrisy here as haemophiliacs were not allowed to be given blood products manufactured from UK paid donors but this safety point was ignored in terms of them receiving factor concentrates made from the plasma of remunerated US donors. So in essence, haemophiliacs received an inferior product, they were treated as second class citizens when it came to both protecting them from viral infection compared to the rest of the UK population receiving blood. These double standards were a key factor covered in documents within the 1991 HIV Haemophilia litigation but sadly the evidence was never heard in court.
Contaminated Blood victims need to know who was responsible for actions taken which affected the safety of patients, therefore, along with plasma pool size, it is important that the Inquiry looks at the implications of using paid donors as to date there has been no accountability for decisions made that led to harm in haemophiliacs and serious loss of life. In addition to haemophiliacs, some partners and children also became infected and many families were left bereaved and have spent years fighting for truth, justice and financial recompense, as, so far, not a penny in compensation has ever been paid.
Update
Today, 12th January 2022, I received the following response to my questions from Dr Rekha Anand, Consultant in Transfusion Medicine, NHSBT
Dear Carol,
Thank you for your enquiry to NHS Blood and Transplant regarding blood donation.
In 1946, the Ministry of Health set up the National Blood Transfusion Service. It relied on the commitment and dedication of voluntary donors, as NHS Blood and Transplant does today. Blood donation has been voluntary since the service was first established in 1946, so there has never been any requirement for us to refer to UK legislation. The blood service in England has never paid donors to give blood or blood component donations.
If you have any further questions, then please do not hesitate to contact me.
Kind regards,
Rekha.
END
Carol Anne Grayson is an independent writer/researcher on global health/human rights/WOT and is Executive Producer of the Oscar nominated, Incident in New Baghdad. She was a Registered Mental Nurse with a Masters in Gender Culture and Development. Carol was awarded the ESRC, Michael Young Prize for Research 2009, and the COTT ‘Action = Life’ Human Rights Award’ for “upholding truth and justice”. She is also a survivor of US “collateral damage”.